
Trial design
Table of Contents
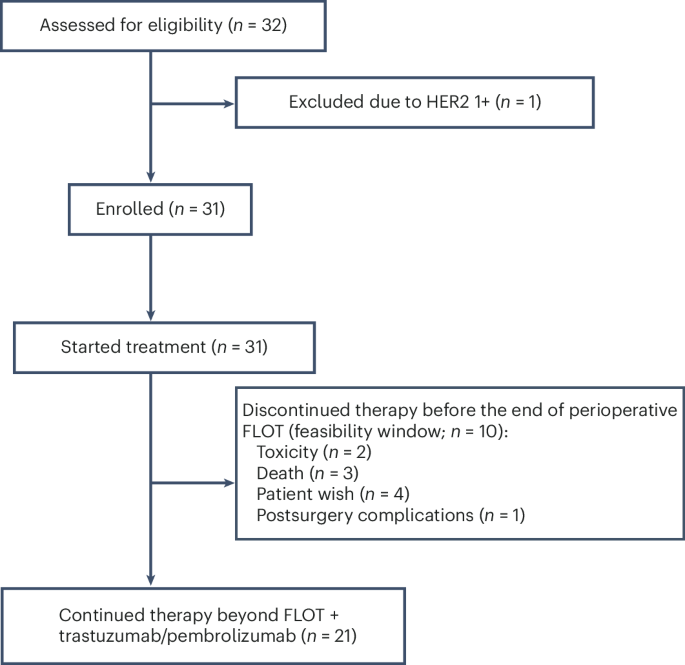
From 17 March 2023 to 7 May 2024, 32 patients were screened and 31 were enrolled across 11 sites in Germany in the open-label, randomized phase 2 IKF/AIO PHERFLOT trial, comprising the intention-to-treat (ITT) population (Fig. 1). The targeted number of patients was 30; therefore, the trial over-recruited by one patient. Key inclusion criteria were nonmetastatic, resectable HER2-positive EGA—defined by immunohistochemistry (IHC) 3+ or IHC 2+ with ISH positivity—located at the gastroesophageal junction (types I–III) or stomach (cT2–4, any N or M0). Key exclusion criteria included prior exposure to immunotherapies, recent major surgery (within 2 weeks), active immunodeficiency, chronic immunosuppression exceeding 10 mg prednisone daily and uncontrolled cardiac conditions (for example, left ventricular ejection fraction < 55%). More information on the trial design, along with a full list of eligibility criteria, is available in the Methods.
An illustration showing the number of patients screened for eligibility, reason for exclusion, the number enrolled and allocated to treatment, and those who either completed or discontinued perioperative therapy during the perioperative FLOT period, defined as the feasibility window. The enrolled cohort (n = 31) represents the ITT population.
Patients were scheduled to receive pembrolizumab (200 mg) and trastuzumab (initial loading dose of 8 mg kg−1followed by 6 mg kg−1) every 3 weeks for 3 cycles before surgery. Concurrent FLOT chemotherapy included docetaxel 50 mg m−2oxaliplatin 85 mg m−2leucovorin 200 mg m−2 and a 24-hour infusion of 5-FU at 2,600 mg m−2administered every 2 weeks for 4 cycles (Extended Data Fig. 1). Surgery was scheduled no earlier than 4 weeks after the final preoperative dose. Postoperatively, patients received 4 additional cycles of the same chemoimmunotherapy, followed by up to 11 cycles of pembrolizumab and trastuzumab alone, totaling 17 cycles over approximately 1 year. The primary endpoints are the pCR rate and the 2-year DFS rate. The trial aimed for a pCR rate greater than 30% and a 2-year DFS rate of over 70%. However, since this paper reports the prespecified interim analysis and the median follow-up time of 14.8 months is too short to assess the 2-year DFS rate, only the pCR rate is reported. Secondary endpoints include the R0 resection rate, overall response rate, OS, feasibility rate (defined as the proportion of patients who did not experience severe toxicity or withdrew from treatment before the final postoperative administration of FLOT plus trastuzumab and pembrolizumab, for reasons other than progressive disease) and safety. Exploratory endpoints include clinical efficacy in molecularly defined subgroups, such as CPS 0 versus 1–9 versus ≥10, HER2-3+ versus HER2-2+/ISH+ and deficient mismatch repair (dMMR) and microsatellite instability-high (MSI-high). In this prespecified interim analysis, only the R0 resection rate, feasibility safety and findings from exploratory molecular and clinical subgroups are reported as secondary endpoints.
Patient and tumor characteristics
Overall 31 patients were recruited to the trial. Despite lack of disease progression, one patient withdrew consent for surgery during neoadjuvant therapy opting for alternative medicine instead of continuing with the protocol. Later, this patient experienced disease progression while off active therapy, thereby excluding a complete response. The median patient age was 65 years (range, 33–76). Most tumors were stage ≥T3 (67.7%) and exhibited lymph node involvement (58.1%; Table 1). All patients had HER2-positive tumors by local pathology, defined as either IHC 3+ or IHC 2+ with ISH positivity; 80.6% of cases were IHC 3+. Histologically, the majority of tumors were of intestinal type (51.6%), followed by diffuse type (9.7%) and mixed histology (3.2%). Signet ring cells were identified in 12.9% of tumors, while 64.5% were negative for signet ring features. With 19.4% of tumors being CPS-negative, the majority were CPS-positive, with 12.9% missing values.
Tumor localization included adenocarcinoma of the esophagogastric junction (AEG) type I (35.5%), AEG type II (32.3%), stomach (22.6%) and AEG type III (9.7%) cancers. Barrett’s esophagus was identified in 22.6% of cases. Tumor grading revealed G2 differentiation in 41.9%, G3 in 38.7% and G1 in 12.9%.
Pathological response
All 30 patients who underwent surgery achieved R0 resection. pCR, defined as Becker TRG1a with no residual lymph node metastasis, was observed in 50.0% (95% CI 31.3–68.7; 15 out of 30) of patients. Subtotal regression (TRG1b) occurred in 20.0% (95% CI 7.7–38.6; 6 out of 30), while partial (TRG2) and minor responses (TRG3) were observed in 10.0% (95% CI 2.1–26.5; 3 out of 30) and 20.0% (95% CI 7.7–38.6; 6 out of 30) of cases, respectively (Fig. 2a). In the ITT population, the pCR rate was 48.4% (95% CI 30.2–66.9; 15 out of 31), subtotal regression occurred in 19.4% (95% CI 7.5–37.5; 6 out of 31), and therefore the major pathological response rate (TRG1a/b) reached 67.7% (95% CI, 48.6–83.3; 21 out of 31). Partial response was observed in 9.7% (95% CI 2.0–25.8; 3 out of 31), minor response in 19.4% (95% CI 7.5–37.5; 6 out of 31) and data were missing in 3.2% of patients (Table 2). Histopathological analysis revealed absence of lymphovascular invasion in 83.3% and no evidence of angioinvasion in 93.3% of resected specimens. Postoperative staging according to American Joint Committee on Cancer (AJCC)/Union for International Cancer Control (UICC) criteria showed tumor downstaging to stage IA or lower in 65.2% (95% CI 42.7–83.6; 15 out of 23) of gastroesophageal junction or distal esophageal tumors and 57.1% of gastric cancers (95% CI 18.4–90.1; 4 out of 7) (Extended Data Tables 1 and 2).

aPathological response distribution in the full cohort according to Becker classification. pCR indicates no residual tumor (TRG1a); subtotal regression (pSR, TRG1b) reflects ≥90% tumor regression; partial response (pPR, TRG2) indicates 50–90% regression; minor response (pMR, TRG3) corresponds to <50% regression. Solid segments indicate minimal regression, while dotted outlines indicate maximal estimated regression according to Becker classification. bpCR rate in patients with available PD-L1 CPS data (n = 27), stratified by CPS 0, ≥1, 1–9 and ≥10. cpCR rate stratified by HER2 expression (HER2 IHC 3+ versus HER2 2+/ISH+). dpCR stratified by tumor stage (T1/2 versus T3/4); one tumor was classified as Tx (n = 30). The complete response rate is depicted by bars, and the upper limit of the 95% CI interval is shown.
Safety
All patients experienced at least one adverse event (AE) (Supplementary Information). Of these, 29 AEs were observed in more than 10% of patients (Table 3). Among the most common AEs of any grade were anorexia (32.3%), constipation (32.3%), diarrhea (83.9%), fatigue (32.3%), nausea (54.8%), decreased neutrophil count (38.7%), peripheral sensory neuropathy (80.6%), weight loss (58.1%) and decreased white blood cell count (48.4%). The most common grade ≥3 AEs were diarrhea (38.7%), decreased neutrophil count (25.8%), sepsis (19.4%) and weight loss (16.1%).
Grade ≥3 treatment-related serious adverse events (SAEs) occurred in 48.4% of patients. Treatment-related SAEs were attributed to pembrolizumab in 32.3% of patients, trastuzumab in 22.6%, oxaliplatin in 41.9%, 5-FU in 48.4%, folinic acid in 29.0% and docetaxel in 41.9% (Extended Data Table 3). The most common grade ≥3 treatment-related AEs were diarrhea, which was attributed to FLOT in 83.3% (10 out of 12) of cases and to pembrolizumab and trastuzumab in 50.0% (6 out of 12); decreased neutrophil count, which was attributed to FLOT in 100% (8 out of 8) of cases and not to pembrolizumab or trastuzumab; and decreased white blood cell count, which was attributed to FLOT in 100% (4 out of 4) of cases and to pembrolizumab and trastuzumab in 50.0% (2 out of 4). No immune-related AEs of special interest or other clinically notable events were observed. Two patients experienced fatal SAEs, both unrelated to the therapy: one died from hyperglycemia and sepsis within 60 days postoperatively, and the other from acute respiratory distress syndrome approximately 3.5 months after surgery (Extended Data Table 4). Moreover, one patient died due to the underlying disease outside the SAE reporting period; the event was unrelated to treatment. Overall, only two patients discontinued therapy due to toxicity during the perioperative FLOT period, defined as the feasibility window. In addition, three patients discontinued due to death, four due to patient preference and one due to postsurgical complications, resulting in a positive feasibility outcome (aimed feasibility rate ≥0.66; see Fig. 1).
Surgery was performed in 30 patients. The mean time to surgery was 88.9 days after enrollment (range, 72–111 days; Extended Data Table 5). The per-protocol window of 4–6 weeks posttreatment was met in 93.3% of cases (28 out of 30). Surgery was complication-free in 70.0% of patients (21 out of 30). Surgical and medical complications were observed in four patients each and one patient showed both surgical and medical complications. Surgical complications included postoperative hemorrhage (n = 1), anastomotic leakage (n = 2), fistula (n = 1), herniation (n = 1) and conduit ischemia (n = 1) (Extended Data Table 6). Medical complications included pneumonia (n = 1), sepsis (n = 1), cardiovascular and respiratory failure with acute respiratory distress syndrome (n = 1), renal failure (n = 1) and other events such as pleural effusion, hemorrhagic shock, staphylococcal infection, worsening of sleep apnea with delirium and peripheral pulmonary embolism (Extended Data Table 7). Overall, eight patients required reoperation (26.7%). The median inpatient stay was 14 days (range, 8–113). No patient died within 30 days postsurgery, but one patient died within 60 days after surgery as described.
Tumor subgroups
PD-L1 expression, measured by the CPS, is a validated biomarker for predicting response to immune checkpoint inhibitors in EGA19,20,21. Similarly, HER2 status serves as a predictive marker for response to HER2-targeted therapies such as trastuzumab19,22,23. CPS data were available for 27 patients. Complete and subtotal responses were observed across CPS 0, CPS 1–9 and CPS ≥ 10 subgroups (Fig. 2b and Table 4). In the group of CPS negative tumors, 33.3% (95% CI 4.3–77.7; 2 out of 6) had a pCR, 50.0% (95% CI 11.8–88.2; 3 out of 6) had a subtotal response and 16.7% (95% CI 0.4–64.1; 1 out of 6) had a partial response (Table 4). In the group of CPS ≥ 1 tumors, 52.4% (95% CI 29.8–74.3; 11 out of 21) had a pCR, 14.3% (95% CI 3.0–36.3; 3 out of 21) had a subtotal response, 28.6% (95% CI 11.3–52.2; 6 out of 21) had a minor response and 4.8% (1 out of 21) did not undergo surgery. In the group of CPS 1–9 tumors, 40.0% (95% CI 12.2–73.8; 4 out of 10) had a pCR, 50.0% (95% CI 18.7–81.3; 5 out of 10) had a minor response and 10.0% (1 out of 10) did not undergo surgery. In the group of CPS ≥ 10 tumors, 63.6% (95% CI 30.8–89.1; 7 out of 11) had a pCR, 27.3% (95% CI 6.0–61.0; 3 out of 11) had a subtotal regression and 9.1% (95% CI 0.2–41.3; 1 out of 11) had a minor response.
Both HER2 IHC 3+ and IHC 2+ with ISH amplification tumors were eligible for inclusion. Among patients with HER2 IHC 3+ expression, the pCR rate was 52.0% (95% CI 31.3–72.2; 13 out of 25), compared to 33.3% (95% CI 4.3–77.7; 2 out of 6) in the HER2 IHC 2+/ISH+ subgroup (Fig. 2c and Table 4). Among patients with lower-stage tumors (T1/2), 77.8% (95% CI 40.0–97.2; 7 out of 9) achieved a complete response, while 11.1% (95% CI 0.3–48.2; 1 out of 9) had a minor response and one declined surgery (Fig. 2d and Table 4). In contrast, among those with T3 or T4 tumors, the pCR rate was 38.1% (95% CI 18.1–61.6; 8 out of 21) and subtotal regression occurred in 28.6% (95% CI 11.3–52.2; 6 out of 21), resulting in a combined major regression rate of 66.7% (95% CI 43.0–85.4; 14 out of 21) in large tumors.
MMR/MSI-status, tested via PCR or IHC, was available for 29 patients; three of these were classified as dMMR by IHC. One of them was MSI stable by PCR, while PCR results were unavailable for the other two. Notably, all three patients with dMMR achieved complete pathological responses.