
Individuals with type 1 diabetes (T1D) have higher risks of cardiovascular disease and chronic kidney disease compared with individuals without diabetes1. Despite advances in glycemic management, 31% and 7% of patients with T1D develop major adverse cardiovascular events (MACEs) and end-stage kidney disease (ESKD) by middle age, respectively2,3. Management of traditional cardiorenal risk factors in T1D remains suboptimal; for example, only 20–30% of patients in the USA achieve the recommended glycemic control targets4,5. New strategies are urgently needed to prevent cardiorenal events in this high-risk population.
Glucagon-like peptide-1 receptor agonists (GLP-1RAs) have demonstrated clinically significant cardiovascular and kidney benefits in individuals with type 2 diabetes (T2D) and cardiovascular benefits in those with obesity and atherosclerotic cardiovascular disease at baseline6,7. However, landmark cardiovascular and kidney outcome trials of GLP-1RAs excluded T1D populations6,7. Evidence in T1D is limited to small, short-term, randomized clinical trials (RCTs) and a few observational studies focusing on surrogate outcomes such as glycemic control and weight loss8,9,10,11,12. Two early trials (ADJUNCT ONE and TWO) showed increased risks of symptomatic hypoglycemia and hyperglycemia with ketosis associated with liraglutide8,9. However, a later trial reported improved safety with continuous glucose monitoring10 and a meta-analysis of 13 RCTs found no increased risk of severe hypoglycemia13. Liraglutide has been the most extensively studied GLP-1RA in T1D, but data on newer agents (semaglutide and tirzepatide) remain limited.
Conducting RCTs evaluating hard cardiorenal outcomes in T1D is challenging due to the young age of this population, with low event rates requiring extended follow-up. Indeed, no RCT has evaluated therapies for the prevention of MACEs or ESKD in T1D. Target trial emulation applies RCT design principles to observational data and can yield conclusions comparable to those of RCTs14. This approach enables timely evaluation of GLP-1RA’s potential effects on major cardiovascular and kidney outcomes in T1D.
Therefore, we conducted a target trial emulation using de-identified electronic health record (EHR) data from Optum Labs Data Warehouse (OLDW) to evaluate the long-term effectiveness and safety of GLP-1RA initiation in T1D. OLDW is a national dataset including ~300 million patients from >60 health systems. The primary outcomes were MACEs (composite of myocardial infarction, stroke or all-cause mortality) and ESKD (dialysis or kidney transplantation). Secondary outcomes included hospitalization for heart failure (HF), major adverse liver events (composite of decompensated cirrhosis, hepatocellular carcinoma or liver transplantation) and weight loss. We included HF and liver outcomes because emerging evidence suggests that GLP-1RAs may improve these outcomes in T2D, partly through weight loss15,16. Similar effects may be plausible in T1D, but data are limited. Safety outcomes were hospitalization for diabetic ketoacidosis (DKA), hospitalization for severe hypoglycemia and gastrointestinal events (composite of biliary disease, pancreatitis, bowel obstruction or gastroparesis).
Consistent with prior sequential target trial emulation studies17we sequentially emulated 135 target trials constructed every consecutive month between January 2013 and March 2024 (Extended Data Fig. 1). Individuals initiating GLP-1RA within the month of enrollment were classified as initiators; all others were noninitiators. Both groups could use other noninsulin glucose-lowering agents within a year before the baseline. The study population included 174,678 individuals with T1D who contributed 6,092,537 person-trials (mean age 43 years, 47% female). Of these, 14,488 person-trials initiated GLP-1RA during a median follow-up of 38 (interquartile range: 18–64) months. Extended Data Table 1 shows baseline characteristics of all person-trials before and after propensity score weighting. After weighting, baseline characteristics were well balanced between groups (all standardized mean differences <10%).
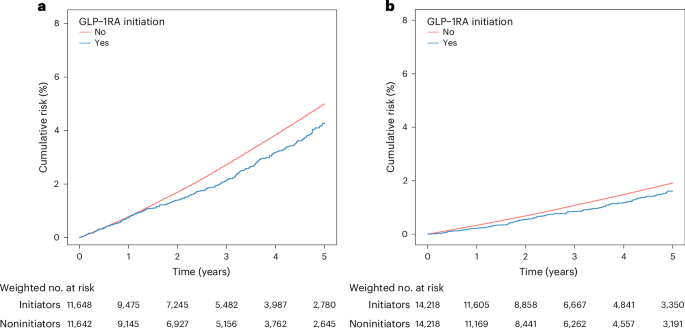
In intention-to-treat analysis of the primary outcomes, the risk of MACEs was lower among GLP-1RA initiators compared with noninitiators, with Kaplan–Meier curves separating after 1.5 years and remaining divergent (Fig. 1a). The 5-year risk of MACEs was 4.3% in the GLP-1RA initiation group and 5.0% in the noninitiation group (risk difference: −0.7% (95% CI: −1.2% to −0.2%)). The overall HR across the study period was 0.85 (95% CI: 0.77–0.95). GLP-1RA initiation was associated with a lower risk of ESKD (Fig. 1b). The risk was 1.6% with GLP-1RA versus 1.9% without at 5 years (risk difference: −0.3% (95% CI: −0.6% to 0.0%)), with an overall HR of 0.81 (95% CI: 0.69–0.95).
In analyses of secondary outcomes, risk of hospitalization for HF was lower with GLP-1RA initiation (HR: 0.82 (95% CI: 0.71–0.94)). GLP-1RA initiation was associated with a lower risk of major adverse liver events (HR: 0.72 (95% CI: 0.60–0.85)). Patients who initiated GLP-1RA were more likely to achieve weight loss of 5%, 10% and 15% (Table 1), with Kaplan–Meier curves diverging within 1 year and remaining separated throughout follow-up (Extended Data Fig. 2c–e).
There was no increased risk of hospitalization for DKA (HR: 0.83 (95% CI: 0.76–0.90)) or severe hypoglycemia (HR: 0.82 (95% CI: 0.72–0.94)) comparing GLP-1RA initiation versus noninitiation. Gastrointestinal events were more frequent in GLP-1RA initiators than in noninitiators, although the risk difference was not statistically significant (Table 1).
In exploratory subgroup analysis, associations between GLP-1RA initiation and lower risks of MACEs, ESKD and major adverse liver events, as well as greater weight loss, were consistent across age (<45 years versus ≥45 years; Extended Data Table 2) and baseline glycated hemoglobin (HbA1c) levels (<8% versus ≥8%; Extended Data Table 3).
In the per-protocol analysis censoring deviation of treatment strategy (median follow-up of 7 months), the results were less precise but consistent with the intention-to-treat results (Extended Data Table 4). The results were similar in sensitivity analyses that applied additional exclusions (no prior hospitalization for outcomes of interest), modified outcome ascertainment (including events with a nonprimary diagnosis), different censoring criteria (censoring at the last body weight measurement for weight changes) and a stricter lab-based T1D definition (Extended Data Table 4). In the sensitivity analysis applying mean imputation for missing covariates, results were consistent (Extended Data Table 4). Using traffic accident as a negative control outcome to assess residual or unmeasured confounding, we found no significant difference between GLP-1RA initiators and noninitiators (HR: 0.96 (95% CI: 0.77–1.20)). E-values were 1.63 for MACEs and 1.77 for ESKD.
In this large, target trial emulation study of youth and adults with T1D, GLP-1RA initiation was associated with significantly lower risks of MACEs and ESKD. Importantly, GLP-1RA initiation was not associated with increased risks of DKA or severe hypoglycemia. These associations were consistent across age and HbA1c subgroups.
Prior GLP-1RA trials in T1D demonstrated short-term effects on HbA1c reduction (0.2–0.5%) and weight loss (3.9–8.8 kg) compared with placebo, but lacked power for long-term outcomes11,12,13. We observed significant risk reductions with GLP-1RA for MACEs (15%) and ESKD (19%). The effect sizes are comparable to the risk reductions observed in T2D trials (13–14% in MACEs and 16% in ESKD)6,7. GLP-1RAs may protect heart and kidneys by reducing inflammation, improving insulin sensitivity and metabolic control, enhancing endothelial function and decreasing platelet aggregation, independent of weight loss18,19. This may explain the similar cardiorenal benefits observed in our study compared with T2D trials, despite the smaller effect size for weight loss.
Our safety findings showed no increased risk of hospitalization for DKA or severe hypoglycemia. These results are consistent with contemporary trials that used continuous glucose monitoring and automated insulin delivery systems10,11,12. Observational studies in T1D also report no increased risk with semaglutide and tirzepatide20,21. Although the glucose-lowering effect of GLP-1RAs may require insulin dose reductions that theoretically increase DKA risk, we did not observe such safety concerns, which may reflect advances in diabetes care. Increased use of diabetes technologies and an evolved understanding of necessary insulin dose adjustments support safer implementation of GLP-1RA therapy in T1D4. Careful patient selection and close monitoring in real-world practice may have also contributed to mitigating safety concerns identified in early trials.
Exploratory subgroup analyses showed generally consistent findings across age groups and HbA1c levels. The observed effectiveness in younger patients is particularly meaningful, because they represent a large portion of the T1D population and face long-term cumulative risk of cardiorenal events. Similarly, consistent cardiorenal benefits across HbA1c levels align with evidence from T2D trials, which demonstrated no treatment heterogeneity by glycemic control6,22. Current guidelines recommend GLP-1RAs for cardiovascular prevention in T2D, regardless of HbA1c levels23. Our results support the consideration of similar therapeutic strategies for all patients with T1D, regardless of age or glycemic status.
GLP-1RA initiation was associated with a 18% lower risk of hospitalization for HF, comparable to the 11–13% reduction seen in T2D trials6,7. This is an important finding in T1D, where HF risk emerges early due to diabetic cardiomyopathy. We observed a 28% lower risk of major liver disease with GLP-1RA initiation. Given that liver disease affects at least 20% of patients with T1D24these hepatoprotective effects represent an important potential benefit of GLP-1RAs. We also found that patients with T1D who initiated GLP-1RAs were 14–25% more likely to achieve clinically meaningful weight loss. This highlights the potential of GLP-1RAs to enhance obesity management—a need that has grown rapidly in both youth and adults with T1D5.
This study has several strengths. We leveraged a large national cohort of patients with T1D with extensive follow-up and applied target trial emulation methodology rigorously to evaluate hard clinical endpoints. We minimized confounding by including numerous patient characteristics and achieving good covariate balance through propensity score weighting. Consistent results across sensitivity analyses and the null association with a negative control outcome (traffic accidents) speak to the robustness of our findings.
This study also has limitations. First, residual and unmeasured confounding is possible. The E-values for MACEs and ESKD suggest that an unmeasured confounder would need to be moderately strong to explain away the observed associations. Second, misclassification of T1D is possible despite using a previously validated algorithm with a high positive predictive value of 88%. However, sensitivity analysis restricted to lab-confirmed T1D cases yielded similar results. Third, hypoglycemia and DKA were identified from hospitalization records, likely capturing only severe cases. However, this ascertainment approach should affect both groups similarly. Fourth, some observed weight loss, especially for 5% weight loss, may have been unintentional (for example, due to illness), which could not be distinguished from intentional weight reduction in EHR data. We did not examine whether observed weight loss was sustainable. Fifth, information on insulin dosing was unavailable, limiting our ability to assess the insulin dose adjustments. Last, although this is one of the largest comparative effectiveness studies of GLP-1RA use in T1D to date, the sample size precluded examination of individual GLP-1RA agents separately or head-to-head comparisons with specific treatments. Future studies are needed to identify the optimal GLP-1RA or dosage for T1D and establish comparative effectiveness against other noninsulin diabetes treatments through active comparator designs.
In this national cohort of patients with T1D, GLP-1RA initiation was associated with lower risks of MACEs and ESKD, without increasing the risks of DKA or severe hypoglycemia. Given the early onset and lifelong burden of T1D, these findings suggest that GLP-1RAs may offer an important strategy to prevent long-term cardiovascular and kidney disease. Large-scale RCTs in people with T1D are warranted to confirm these findings.