
Country classification
Table of Contents
- Country classification
- Site-specific proportions of gastric cancer
- Source of gastric cardia and noncardia cancers
- Number of gastric cancers attributable to H. pylori infection
- Expected lifetime number of gastric cancers
- Sensitivity and stratified analyses
- Ethics and inclusion statement
- Reporting summary
We present the contribution to the expected absolute burden of gastric cancer in the year 2022 of the 185 countries included in IARC’s GLOBOCAN database hosted at the Global Cancer Observatory42grouped by continent, UN world region and level of HDI. The HDI is reported by the UN Development Programme (https://hdr.undp.org/data-center) as a measure of the social and economic development of countries; details on the data sources and methods used in developing the GLOBOCAN estimates at the national level are available elsewhere43. Countries were sorted by the expected number of cases and subsequently grouped into the following five categories of incidence burden: >1,000,000, 100,000–1,000,000, 35,000–100,000, 10,000–35,000 and <10,000. We also grouped countries based on their age-standardized incidence rates to illustrate the gastric cancer burden: 0–5 in 100,000, >5–10 in 100,000 and >10 in 100,000. The HDI was further stratified by the predefined UN Development Programme four-tier categories into the low (<0.55), middle (0.55–0.70), high (0.70–0.79) and very high (≥0.80) levels.
Site-specific proportions of gastric cancer
To take into account the current evidence on potentially differential relationships between H. pylori infection and gastric cancer subsite by region28we obtained the site-specific proportions of gastric cancer from the CI5-XII database44 for 52 countries where subsite classification is available, including a ‘cardia’ category (C16.0). Previous versions of the CI5 were used if no information was available in CI5-XII at the country level (ten countries), and other cancer registry data were used for eight other countries (see below for details).
Source of gastric cardia and noncardia cancers
Country-specific (when available) and subregional proportions of CGC versus NCGC were based on the following:
-
CI5-XII for Algeria, Australia, Austria, Belarus, Belgium, Benin, Brazil, Canada, Chile, China, Colombia, Costa Rica, Croatia, Cyprus, Czechia, Denmark, Ecuador, Estonia, Finland, France, Germany, Guadeloupe, Iceland, Iran, Ireland, Israel, Italy, Japan, Latvia, Lithuania, Malta, Martinique, Netherlands, New Caledonia, New Zealand, Norway, Peru, Poland, Portugal, Puerto Rico, Russia, Réunion, Singapore, Slovenia, South Korea, Spain, Sweden, Switzerland, Turkey, Ukraine, the UK and the USA
-
CI5-XI for Bulgaria, French Guiana, Jamaica, Jordan, Saudi Arabia, Slovakia and Vietnam
-
CI5-X for Egypt, Qatar and Tunisia
-
Other cancer registry data with at least 25% of topographically specified cases for French Polynesia, Kazakhstan, Nigeria, South Africa, Pakistan, Romania, Serbia and Vanuatu
When country-specific estimates from the proportions of cardia and noncardia cancers were not available, we attributed the mean values of the UN subregional proportions estimated from a hierarchical logistic random-effects model.
The ‘noncardia’ category includes six different topographic locations (C16.1 to C16.6), plus an overlapping category (C16.8) and a ‘not otherwise specified’ category (C16.9). The estimated numbers of noncardia cancer cases were obtained by applying the proportion of NCGC cases in existing local cancer registries (that is, C16.1 to C16.9) to the total number of gastric cancer cases by sex, age groups (<65 and 65+ years) and world area as estimated in the GLOBOCAN database, given that subsite data are not available. Using this method, we made the strong assumption that all cases in C16.8 and C16.9 are noncardia. To compute the proportions, we considered only the registries with at least 25% of topographically specified cases (C16.0 to C16.8). The proportions of CGC and NCGC were estimated using country-specific data for those with more than four cases of gastric cancer per age group and sex. Country-specific data were pooled at the UN subregional level to estimate the proportion of cardia and noncardia cases for countries with insufficient data. More details are available elsewhere45. To assess the robustness of our estimates to the cancer registry selection, we reconducted the analysis including the following 30 additional countries where registries had <25% of topographically specified cases: Argentina, Bahrain, Bosnia and Herzegovina, Botswana, Brunei, Congo (Brazzaville), Cuba, Côte d’Ivoire, Ghana, Guinea, India, Kenya, Kuwait, Lebanon, Libya, Malawi, Malaysia, Mali, Mauritius, Morocco, Namibia, Oman, Philippines, Seychelles, Thailand, Trinidad and Tobago, Uganda, Uruguay, Zambia and Zimbabwe. The results did not materially change.
Number of gastric cancers attributable to H. pylori infection
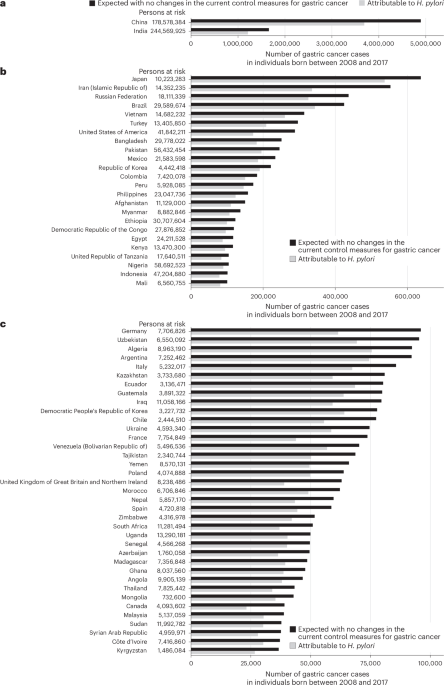
Accurate quantification of the fraction of gastric cancer cases attributable to H. pylori is highly dependent on obtaining accurate estimates of relative risk. In this study, we used data from improved studies that assessed the relative risk using prediagnostic samples with long-term follow-up, as well as studies using more sensitive immunoblotting than ELISA, to be consistent with our previous work on the global burden of cancer attributable to infections12,46. The estimated number of gastric cancer cases attributable to chronic infection with H. pylori was obtained using the attributable fractions previously calculated from prospective studies that applied immunoblotting to detect H. pylori at least 10 years before cancer diagnosis46separately for NCGC (89% worldwide) and CGC (29% in eastern Asia, 0% in the rest of the world)12except for China for which we used the latest estimates from a more recently published large-scale prospective study (78.5% for NCGC and 62.1% for CGC)29. These H. pylori-attributable cases are assumed to be potentially preventable through implementing population-based H. pylori screen-and-treat programs. Of note, H. pylori infection rates were not incorporated into our analyses, as we assumed no change in the current practices of gastric cancer prevention and no change in age-specific gastric cancer incidence rates in future years.
Expected lifetime number of gastric cancers
We estimated the expected lifetime number of gastric cancers among ten birth cohorts aged 5–14 years in 2022 (that is, those born between 2008 and 2017), up to the time point when the individuals would reach 84 years old, by adapting ATLAS, a previously published cancer progression model47. The statistical package for the ATLAS model is implemented in the methis.atlas R package. More information about the model is available on the IARC’s METHIS website (https://iarc-miarc.gitlab.io/methis/methis.website/docs/models/atlas.html). ATLAS combines the age-specific incidence estimates from the Global Cancer Observatory GLOBOCAN (https://gco.iarc.fr//today/en) project and the cohort-specific mortality rate projections by age from the UN Department of Economic and Social Affairs, Population Division, allowing for the competing risk of dying from any cause before being diagnosed with gastric cancer. Accounting for cohort-specific mortality rates by age enabled us to incorporate future demographic changes in our projections.
Briefly, for a given cohort, the expected cumulative number of gastric cancers between age 5 and 84 years was calculated using the 5-year age group-specific gastric cancer incidence rate projections from GLOBOCAN 2022, and 5-year age group-specific mortality rates were obtained from the UN Department of Economic and Social Affairs, Population Division48.
Let A5 be the age group 5 years and A84 the age group 84 years. Let us denote by lC and lM the gastric cancer incidence rate and mortality rate, respectively, both assumed to be piecewise constant functions in each 5-year age group. That is, for i = 5, …, 84, lC,i and lM,i denote the constant Ai-specific gastric cancer incidence and mortality rates, respectively. Let us also designate by ({A}_{i}^{textrm{L}}) and ({A}_{i}^{textrm{U}}) the lower and upper bounds of age interval Aiwith, for i > 0, ({A}_{i}^{textrm{L}}={A}_{i-1}^{textrm{U}}). Then, the survival free from an event (that is, gastric cancer diagnosis or death) by age ({A}_{I}^{textrm{U}}) for a cohort of individuals aged 5 years at the start of follow-up can be calculated according to the following formula:
$$begin{array}{l}Sleft({A}_{I}^{textrm{U}}right)=Sleft({A}_{I+1}^{textrm{L}}right)=exp left(-{int}_{!{A}_{0}^{textrm{L}}}^{{,{A}_{I}^{textrm{U}}}}left({lambda}_{textrm{C}}left(uright)+{lambda}_{textrm{M}}left(uright)right){{textrm{d}}u}right)qquadqquadqquadquadqquad,=exp left(-5mathop{sum}limits_{i=0}^{I}left({lambda}_{{textrm{C}},i}+{lambda}_{{textrm{M}},i}right)right)end{array}$$
Now, the cumulative incidence of gastric cancer by age ({A}_{I}^{textrm{U}}) can be calculated as
$${textrm{CumI}}left({A}_{I}^{textrm{U}}right)={int}_{{!A}_{0}^{textrm{L}}}^{{{A}_{I}^{textrm{U}}}}{lambda}_{textrm{C}}left(uright)Sleft(uright){{textrm{d}}u}=mathop{sum }limits_{i=0}^{I}{lambda }_{{textrm{C}},i}{int}_{{!A}_{i}^{textrm{L}}}^{{{A}_{i}^{textrm{U}}}}Sleft(uright){{textrm{d}}u}=mathop{sum }limits_{i=0}^{I}{textrm{CumI}}_{i}$$
We then have
$$begin{array}{ll}{rm{CumI}}_{i}={lambda}_{{rm{C}},i}{displaystyleint}_{!{A}_{i}^{rm{L}}}^{{{A}_{i}^{rm{U}}}}Sleft(uright){{rm{d}}u}qquadquad={lambda }_{{rm{C}},i}{displaystyleint }_{!{A}_{i}^{rm{L}}}^{{{A}_{i}^{rm{U}}}}exp left(-{displaystyleint }_{!{A}_{0}^{rm{L}}}^{{u}}left({lambda }_{rm{C}}left(vright)+{lambda }_{rm{M}}left(vright)right){{rm{d}}v}right){{rm{d}}u}qquadquad={lambda }_{{rm{C}},i}{displaystyleint }_{!{A}_{i}^{rm{L}}}^{{{A}_{i}^{rm{U}}}}exp left(-{displaystyleint }_{!{A}_{0}^{rm{L}}}^{{{A}_{i}^{rm{L}}}}left({lambda }_{rm{C}}left(vright)+{lambda }_{rm{M}}left(vright)right){{rm{d}}v}right)qquadquadquad;exp left(-{displaystyleint }_{!{A}_{i}^{rm{L}}}^{{u}}left({lambda }_{rm{C}}left(vright)+{lambda }_{rm{M}}left(vright)right){{rm{d}}v}right){{rm{d}}u}qquadquad={lambda }_{{rm{C}},i}exp left(-5mathop{sum }limits_{k=0}^{i-1}left({lambda }_{{rm{C}},k}+{lambda }_{{rm{M}},k}right)right){displaystyleint }_{!{A}_{i}^{rm{L}}}^{{{A}_{i}^{rm{U}}}}qquadquadquad;exp left(-{displaystyleint }_{!{A}_{i}^{rm{L}}}^{{u}}left({lambda }_{rm{C}}left(vright)+{lambda }_{rm{M}}left(vright)right){{rm{d}}v}right){{rm{d}}u}qquadquad=-displaystylefrac{{lambda }_{{rm{C}},i}}{{lambda }_{{rm{C}},i}+{lambda }_{{rm{M}},i}}exp left(-5mathop{sum }limits_{k=0}^{i-1}left({lambda }_{{rm{C}},k}+{lambda }_{{rm{M}},k}right)right)qquadquadquad;left(exp left(-5left({lambda }_{{rm{C}},i}+{lambda }_{{rm{M}},i}right)right)-1right)qquadquad=-displaystylefrac{{lambda }_{{rm{C}},i}}{{lambda }_{{rm{C}},i}+{lambda }_{{rm{M}},i}}left(Sleft({A}_{i}^{rm{U}}right)-Sleft({A}_{i-1}^{rm{U}}right)right)qquadquad=displaystylefrac{{lambda }_{{rm{C}},i}}{{lambda }_{{rm{C}},i}+{lambda }_{{rm{M}},i}}left(Sleft({A}_{i}^{rm{L}}right)-Sleft({A}_{i}^{rm{U}}right)right)end{array}$$
Based on the assumption that the age group-specific incidence rates were stable across birth cohorts, the cumulative incidence between ages 5–14 years in 2022 and age 84 years was then obtained by summing the age group-specific contributions: ({rm{Cum}}{{rm{I}}}_{5-84}={sum }_{i=5}^{84}{rm{Cum}}{{rm{I}}}_{i}). Finally, the cumulative number of gastric cancer cases was calculated by multiplying this cumulative incidence by the size of the cohort at age 5–14 years in 2022, estimated from the UN database. UIs were estimated with Monte Carlo simulation combining the uncertainty about the overall gastric cancer incidence as reported in GLOBOCAN 2022 (central estimates and 95% UI), age-specific distribution of gastric cancer (GLOBOCAN 2022), proportions of CGC and NCGC, and mortality rate prediction uncertainties as reported by the UN Population Division (median estimates and 95% UI).
To illustrate the effect of future demographic changes on country-specific gastric cancer burden, we compared the average number of lifetime gastric cancer cases (up to age 84 years) that would be expected in an average single birth cohort born between 2008 and 2017—assuming no changes in the current practices of gastric cancer prevention—versus the total number of cases as estimated in the GLOBOCAN database, calculating a ratio between the two estimates (termed as the ‘ratio of change’). We assumed no change in the annual incidence of gastric cancer attributable to modifications in H. pylori prevalence or gastric cancer screening practices. The correlation between the above-mentioned ratio of change and country-specific HDI was calculated using Pearson’s coefficient (r). Country-specific 95% UIs for the average number of expected cases, obtained using simulation, combine the uncertainty in the gastric cancer incidence estimates from GLOBOCAN 2022 (central estimates and 95% UI) and all-cause mortality projections from the UN (median variant and 95% UI). These two sources of uncertainty are considered independent. No trends in age-specific gastric cancer incidence rates are considered.
Sensitivity and stratified analyses
We additionally conducted sensitivity analyses to quantify how much our estimates are affected by varying patterns of disease burden, life expectancy and cancer control practice. We also performed stratified analyses by sex and world region. The lifetime number of gastric cancers was estimated according to different model parameter disruptions in the 2008–2017 birth cohorts. Model outcomes were compared to the reference scenario, that is, (1) no competitive risk between CGC and NCGC, (2) median UN death rate scenario, (3) no APC in the incidence of CGC and NCGC, and (4) no change in the current public health intervention for gastric cancer control. The estimates were expressed in terms of the ratio of change and the percentage of change in the lifetime number of gastric cancer cases expected. The tested parameters included the following: (1) competing rate of the CGC versus NCGC burden; (2) death rate incorporating the lower 95% (optimistic) versus the higher 95% (pessimistic) estimates of the probabilistic projection of crude death rate by country or area in 2024–2100 from the UN model; (3) APC in the incidence of CGC and NCGC for 10 and 20 years, separately, by applying varying levels of APC (−3% to 3%); and (4) population-level impact of H. pylori screen-and-treat strategies by 80–100%.
All analyses were conducted with R (version 4.4.1) and the methis.atlas package (version 0.3.0).
Ethics and inclusion statement
This study was conducted with a commitment to providing policymakers with evidence that is both globally comparable and regionally meaningful. GLOBOCAN and CI5 estimates are based on data from population-based cancer registries and vital statistics registries worldwide, including low- and middle-income countries, and are relevant to all countries. Global estimates generated through this research are designed to be actionable and relevant to regional policymakers, providing them with timely, high-resolution data to inform decision-making and prioritize interventions tailored to local needs.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.