
Description of study participants
Table of Contents
The characteristics and genotypes of the patients enrolled in the study are shown in Table 1. A total of nine patients were enrolled in the trial (two with SD and seven with TSD; NCT04669535 and NCT06614569). There were two screen failures: one because of a temporary hold that was placed on enrollment, which was eventually lifted and the participant was re-enrolled as Patient 005; and one because of rapid clinical worsening of the patient’s condition immediately before planned enrollment. Our study design did not exclude patients who showed seropositivity for the AAVrh8 capsid. We noted that only Patient 002 showed seropositivity, but we did not assess whether this affected patient outcomes. Because this trial was designed to study both safety and biological activity in infantile patients with GM2 disease, bioactivity and functional outcome measures in the infantile patients were the primary focus. Because of safety events in juvenile patients, they were excluded from further enrollment and not included in further analysis of outcomes.
General safety
With respect to general safety, there were a total of 171 adverse events (AEs) recorded during the study, of which only 15 were found to be possibly or definitely related to the vector (see Supplementary Table 1 for a complete list of AEs and clinical laboratory findings). Distribution of the 15 potentially vector-related AEs by dose and severity is shown in Table 2. Of these AEs, nine consisted of elevated liver enzymes and/or elevated anti-capsid interferon-ɣ enzyme-linked immunosorbent spot (ELISpot) responses, and these responses were seen at low, medium and high dose levels. All AEs of this type responded to increased steroid dosages with subsequent reduction in both transaminase levels and numbers of spot-forming units by ELISpot12. Two patients who were enrolled in this study died after being treated. Patient 001 died at study day 805 from disease progression and patient 002 died at study day 163 from fulminant, hemorrhagic Clostridioides difficile infection secondary to prolonged hospitalizations and antibiotic use because of underlying disease progression. This was deemed to be unrelated to the vector, surgery or protocol medications.
Interestingly, two of three juvenile patients noted new or worsening dystonia, and the third experienced unexpected progression of the neurologic manifestations of their GM2 gangliosidosis. This type of AE was not observed in any of the infantile patients. The worsening of dystonia developed between one and two months after thalamic injection, suggesting that it could possibly be related to the biology of transgene expression in the thalami or adjacent basal ganglia structures. Although the precise mechanism of this phenomenon is not clear, neurotransmitter metabolites were measured in the CSF to determine whether either surgical process or vector effects adjacent to the basal ganglia in the juvenile patients with GM2 gangliosidosis altered the function of neurons in basal ganglia structures (Supplementary Table 2). Once the observation of dystonia was made in juvenile patients, only infantile patients were recruited for the remainder of the study.
Safety and confirmation of BiT convection-enhanced delivery
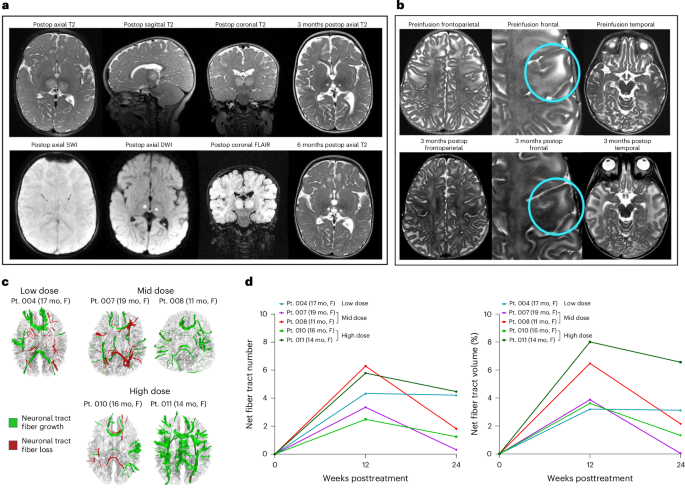
To confirm thalamic infusion and evaluate for any acute toxicity, each participant underwent cranial magnetic resonance imaging (MRI) without contrast within the first 30 min following the end of vector infusion. In eight of nine BiT infusions, there was a change in signal associated with T2-FLAIR hyperintensity in the thalamus indicative of the accuracy of the infusion sites (Fig. 1a). We noted that Patient 004 did not demonstrate an increase in T2-FLAIR signal in the thalami postinfusion, which is possibly related to backflow of infusate into the subarachnoid space. There were no clinically significant surgical complications such as surgical tract-related intracerebral hemorrhage, cerebral edema or parenchymal tissue injury in the thalamus. Both patients in the high-dose cohort (1,250 μl in each thalamus) displayed foci of T2 hyperintensity in the thalami related to the site of the catheter tip (Extended Data Fig. 2). One patient had a clinically insignificant radiological area of ischemia (as demonstrated by increase in diffusion-weighted imaging signal) in the right caudate nucleus close to the catheter trajectory, which was associated with a mild volume loss in that region in MRI data at 3 and 6 months postinfusion.
aImmediate postoperation (postop) MRI depicting BiT injection of AAVrh8-HEXA and AAVrh8-HEXB (1,250 μl and 4.1 × 1013 vector genomes (vg) per thalamus). MRI without contrast showing T2-FLAIR hyperintensity in the thalamus at the injection site. The hyperintensity decreases over time (at 3 and 6 months). There is no evidence of hemorrhage or other major complication associated with the injection. bTwo patients demonstrated an increase in cortical T2 hypointensity, suggestive of myelin production, over the course of three months postinfusion. The effect was observed in the frontoparietal cortex, but not in the temporal cortex. cDTI for five patients taken at baseline and 24 weeks after treatment showing neural tract fiber growth (green) and loss (red). dQuantification of percent change in tract fiber numbers and volume from DTI data at 12 and 24 weeks posttreatment. DWI, diffusion-weighted imaging; F, female; mo, months, Pt., patient; SWI, susceptibility-weighted imaging.
Sixteen AEs were deemed to be potentially related to the BiT convection-enhanced delivery procedures and/or the associated anesthesia (Table 2). The most frequent surgical complications were related to delayed wound healing. These included superficial wound dehiscence after suture removal requiring placement of reinforcement sutures in some circumstances. After wound dehiscence was observed in the first few patients, the study protocol was amended and the time until suture removal was lengthened from 2 to 3 weeks.
Neuroimaging efficacy
The MRI data suggest a therapeutic effect of the treatment. Specifically, there was one patient in whom myelination in the frontal lobe white matter was improved (Fig. 1b), another in whom myelination was marginally improved and a more consistent finding of preservation of myelination in the cerebral cortex. The temporal lobe white matter did not show signs of this potentially beneficial effect. Vector-treated patients showed a slower increase in total brain volume than historical controls, potentially indicating a therapeutic effect on the macrocephaly, which is characteristic of this disease (Extended Data Fig. 3 and Extended Data Tables 1 and 2). There was positive correlation between lower brain volume and a lower global clinical severity score as well (Extended Data Fig. 3 and Extended Data Tables 1 and 2). These findings are consistent with a positive therapeutic effect, although this is not conclusive.
There was evidence of development of new myelinated tracts after vector treatment by DTI. Two DTI parameters, fractional anisotropy (FA) and radial diffusivity, showed trends indicative of increased myelination in the lentiform nucleus (putamen and globus pallidus), but not in other brain regions such as the temporal lobe (Extended Data Fig. 4). Poor AAV distribution to the temporal lobes has previously been reported in preclinical large animal studies9,13,14. In addition, DTI data were analyzed by differential tractography to map newly myelinated neural tracts in six of the vector-treated patients (Fig. 1c,d). As shown by the green pseudocolor in Fig. 1cfunctional white tracts were observed across cerebral lobes and frequently in the corpus collosum at 12 weeks after treatment, while fewer such tracts were seen at 24 weeks posttherapy. However, all six patients had positive net fiber tract metrics at both visits, indicating improved myelination.
Clinical laboratory and immunologic assessments
As previously reported in patients with TSD, elevations in transaminase values were observed in most patients before gene transfer15. However, following gene delivery there were further significant increases from baseline in each patient. These were associated temporally with positive results on the ELISpot assay designed to evaluate effector T cell responses to AAVrh8 capsid epitopes (Fig. 2). In each case, the patients were treated by increasing the corticosteroid dosage levels, either from 1 mg kg−1 daily to 2 mg kg−1 daily prednisolone or by adding a 3-day course of methylprednisolone at 10 mg kg−1 d−1 before returning to a 2 mg kg−1 d−1 prednisolone dosage (Supplementary Table 3). Transaminase elevations from baseline ultimately resolved in all participants, as did the number of spot-forming units on capsid ELISpot assays. All participants’ serum neutralizing antibody titers to AAVrh8 increased by more than tenfold following the therapy12.

Normal ranges are indicated for liver enzymes in dotted lines. Positive and negative ELISpot responses are denoted by red and blue shading, respectively. Complete immune response data are presented in the companion publication12. ALT, alanine transaminase; AST, aspartate aminotransferase; GGT, gamma-glutamyl transferase; IFNɣ, interferon-ɣ; M, male; NA, not applicable (no sample collected); yr, years.
Bioactivity outcomes
The combined rAAV8-HexA and rAAV8-HexB vector was designed to express both subunits of the functional HexA enzyme. HexA activity was measured in CSF samples taken from all patients before dosing on day 2 (after BiT delivery, just before intra-CM and IT delivery), at 12 weeks and at 24 weeks after gene therapy to determine whether enzyme activity was increased in the CNS. Patients in the earlier cohort provided samples at additional time points.
As shown in Fig. 3athere was a clear dose–response relationship for HexA enzyme activity among the infantile patients with TSD (the CSF HexA assay is uninformative in patients with SD, who are deficient in the beta subunit of HEXAbecause homodimers of the alpha subunit of the HEXA gene product are able to hydrolyze the substrate used in the assay), with the highest CSF HexA enzyme activity being 0.59 nm h−1 ml−1 in the final participant (Patient 011) at the 12-week time point, which is 13% of the normal value. Overall, HexA activity levels peaked in most participants at 12 weeks and declined somewhat thereafter, but remained above pretreatment levels throughout the duration of the study (Fig. 3a). Similarly, the total Hex levels in the serum of infantile patients with TSD increased after vector treatment, peaking between day 22 (exceeding 40 nm h−1 ml) and week 8, and then partially declining (Fig. 3B). As with the CSF HexA activity, the highest Hex levels in the serum were observed in the high-dose cohort, indicating a dose–response relationship for biological activity. Finally, C18:0 and C20:0 GM2 levels were quantified by mass spectrometry in CSF and correlated with HexA levels at the same time points. As observed in previous studies16the C20:0 GM2 levels were more consistently lowered in vector-treated participants than C18:0 GM2 (Fig. 3c and Supplementary Table 4).

aHexA enzyme activity in CSF collected at the indicated time points. Analysis for HexA enzyme was only interpretable in patients with TSD. bTotal serum Hex levels collected at the indicated time points. The dashed line indicates normal Hex levels. cC20:0 GM2 quantification by mass spectrometry. We note that juvenile patients have lower levels of GM2 as predicted by their disease subtype. dCSF HexA activity levels from a generally correlated with GM2 20:0 levels.
Measurement of CSF GM2 20:0 by mass spectrometry did not show consistent dose-related differences from pre- to posttreatment. However, of the six infantile patients in the study, four showed a downward trend in GM2 20:0 (Extended Data Table 1). The percentage decrease of CSF GM2 20:0 from the baseline to its lowest point ranged from a 9.1% decrease in one patient in the low-dose cohort to a 52.5% decrease in one patient in the mid-dose cohort and 49.5% in one patient in the high-dose cohort. Two participants reached the lowest level (nadir) of recorded concentration of GM2 20:0 at 12 weeks and two reached their minimum value at 24 weeks; one showed two nadirs at 12 and 48 weeks. This time frame was generally concurrent with the timing of the highest levels of CSF HexA activity (Fig. 3D).
Neurologic and developmental outcomes
Patients with GM2 gangliosidosis have a substantial increase in both brain and ventricle volume over time, which is thought to be caused by the accumulation of GM2 gangliosides17. The patients in this study demonstrated a slower rate of brain volume growth (measured in ml per year) compared with historical data of age-matched patients with GM2 gangliosidosis, potentially indicating a therapeutic effect on the macrocephaly, which is characteristic of this disease (Extended Data Figs. 3 and 5Extended Data Table 2 and Supplementary Table 5). There was no significant decrease in growth of ventricle volume for the patients in this study, and so the change cannot be explained by atrophy alone. As with other biomarkers, there was a correlation between lower brain volume and less-severe Clinical Global Inventory (CGI) scores. We noted that the two patients from the high-dose cohort showed an overall decrease in cerebellar cortex volume following treatment, while the remaining study participants did not (Extended Data Fig. 5). These findings are consistent with a positive therapeutic effect, although this is not conclusive.
The complete set of assessments including neurologic and developmental outcomes is presented in Extended Data Fig. 6. Changes in GCI score from baseline for infantile patients are shown in Fig. 4A. Patients 007 and 008 (both mid dose) showed improvement from baseline at 4 weeks. Patient 010 (high dose) maintained baseline score at the 4- and 12-week time points, but then declined. Patient 011 (high dose) improved from baseline at 12 weeks and maintained that improvement at 24 weeks (which was the end of the study for this participant). Of note, this patient had the highest posttreatment CSF HexA activity. As shown in Fig. 4Athere was a strong negative correlation between vector dose and the last recorded CGI value. All participants were stable on this score at 4 weeks, with Patients 007 and 008 worsening at week 12 and thereafter. All other patients maintained the same severity score at week 24.

aCGI severity scores at each time point. Lower scores indicate better neurological status. b,cInfantile patients’ neurologic exam scores for seizure severity (b) and sucking or swallowing (c). A higher score indicates worsened severity.
Infantile neurologic exam scores for seizures and swallowing
Two important aspects of infantile disease progression include the frequency and severity of seizures and retaining the ability to suck and/or swallow so that patients may maintain oral feeding. As shown in Fig. 4BPatient 011 was seizure-free for the entire duration of the study (24 weeks), but developed seizures shortly after the end of the study period. Patient 010 had an electroencephalogram (EEG) showing seizure activity before treatment but was placed on Keppra and remained stable on Keppra alone to the end of the study (24 weeks). With respect to the ability to suck and/or swallow without aspiration, all participants were either stable or improved (Patients 010 and 011) (Fig. 4c). For both patients in the high-dose cohort, the ability to feed orally was maintained at the end of the study (24 weeks).