
Study design, procedures and participants
Table of Contents
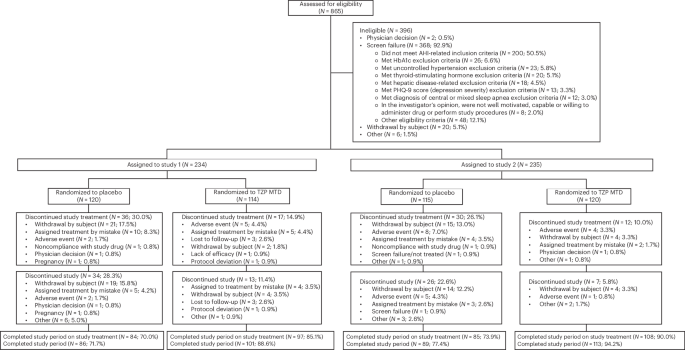
The SURMOUNT-OSA program included two 52-week, randomized, placebo-controlled phase 3 studies. Study 1 included participants who were unwilling or unable to use PAP therapy, and study 2 included participants who had been using PAP therapy for at least 3 months at screening, and who planned to continue PAP for the duration of the trial. Participants were randomly assigned in a 1:1 ratio to receive either tirzepatide at the maximum tolerated dose (10 or 15 mg) or placebo once weekly. The SURMOUNT-OSA program was registered at ClinicalTrials.gov (NCT05412004), and the two studies’ full design, key eligibility criteria, procedures and primary efficacy and safety results have been published previously13,14. Participants were screened and enrolled irrespective of their sex. Sex was self-reported by participants.
Objectives
First, this analysis investigated the association of tirzepatide with changes in cardiometabolic risk markers in participants with moderate-to-severe OSA and obesity. Second, the analysis estimated the relative contribution of weight loss, AHI and SASHB reduction to the improvement in cardiometabolic characteristics of subjects treated with tirzepatide.
Parameters measured included change from baseline in SBP, DBP and levels of hsCRP, HDL-C, non-HDL-C, triglycerides, LDL-C, VLDL-C, fasting insulin and HOMA-IR, in tirzepatide versus placebo.
Mediation analysis was performed to estimate the proportion of tirzepatide treatment-associated changes in cardiometabolic risk measures due to either an effect of weight reduction or an effect of changes in sleep-disordered breathing measured by AHI and SASHB. SASHB is a cumulative measure of oxygen desaturation associated with apneas and hypopneas which, in observational studies, predicted OSA-related cardiovascular mortality and morbidity better than AHI40,41.
For each cardiometabolic risk measure, three analyses were performed: estimation of the proportion of efficacy mediated by change from baseline in body weight, change from baseline in AHI and SASHB and, lastly, change from baseline in all three mediators combined.
Improvements in these mediators with tirzepatide treatment compared with placebo from SURMOUNT-OSA studies have been previously published and are as follows:
ETD between tirzepatide and placebo in study 1 was −16.1% (95% CI −18.0 to −14.2) for body weight, −20.0 events per hour (95% CI −25.8 to −14.2) for AHI and −70.1%min h−1 (95% CI −90.9 to −49.3) for SASHB13. ETD between tirzepatide and placebo in study 2 was −17.3% (95% CI −19.3 to −15.3) for body weight, −23.8 events per hour (95% CI −29.6 to −17.9) for AHI and −61.3%min h−1 (95% CI −84.7 to −37.9) for SASHB13.
Statistical analysis
Changes in SBP, DBP and hsCRP from SURMOUNT-OSA have already been reported using treatment-regimen estimand analysis13. The analyses reported here were guided by the ‘efficacy’ estimand; the analysis included data collected before permanent discontinuation of study intervention and was conducted using the efficacy analysis set. For efficacy analysis, missing values were imputed using multiple imputation based on the reason of intercurrent events. All results are reported using the efficacy estimand unless otherwise specified.
Unless otherwise noted, all tests of treatment effects were conducted at a two-sided alpha level of 0.05, and the CIs were calculated at 95%. In statistical summaries and analyses, participants were analyzed as randomized.
The mixed model repeated measures analysis, a restricted-maximum-likelihood-based model, was used to analyze continuous longitudinal variables. All the longitudinal observations at each scheduled postbaseline visit were included in the analysis. The model includes the fixed class effects of treatment, strata (pooled country/geographic region, baseline OSA severity and gender), visit and treatment-by-visit interaction, as well as the continuous, fixed covariate of baseline value. The significance tests were based on least-squares means and type III tests. As all of these endpoints were exploratory in nature, the P values were not adjusted for multiplicity. Statistical analyses were performed using SAS version 9.3.
Mediation analyses were conducted to decompose the total effect of tirzepatide on cardiometabolic risk markers into direct effect and indirect effect. The direct effect quantified the effect of tirzepatide versus placebo on change in cardiometabolic outcomes, independent of changes in mediators. Conversely, the indirect effect captured the effect of tirzepatide versus placebo on change in cardiometabolic outcomes associated with changes in mediators. Because these comparisons involve non-observable counterfactual scenarios, natural effect models were employed to estimate the direct and indirect effects42. The total effect was defined as the sum of these two components. The proportion mediated was calculated as the indirect effect divided by the total effect then multiplying by 100%, and the standard errors were derived using the bootstrap method. The mediation analyses were performed on the pooled study 1 and study 2 populations. The outcome was the change in cardiometabolic risk measure from baseline to the end of the study. Analyses on SBP and DBP were performed on the original scale, and analyses on hsCRP, HDL-C, non-HDL-C, triglycerides and HOMA-IR were performed on the log scale. Baseline covariates included region, sex, baseline cardiometabolic risk measure, AHI, body weight and log-transformed SASHB. We investigated the effects of mediators for three scenarios: first, a single mediator of change from baseline in body weight; second, two independent mediators of change from baseline in AHI and change from baseline in SASHB to represent changes attributable to OSA severity improvement; and lastly, a combination of the effect of changes in body weight, AHI and SASHB as three parallel mediators. The post-treatment confounders were controlled for and included change in AHI and SASHB when the mediator was change from baseline in body weight and change in body weight when the mediator was change from baseline in AHI and SASHB. No post-treatment confounders were controlled for when all of the change from baseline in body weight, AHI and SASHB were mediators. Log transformation was always applied for SASHB. The mediation analyses were performed using the ‘CMAverse’ package version 0.1.0 in R version 4.1.2 (ref. 42).
Pearson’s correlation coefficients were also calculated between the cardiometabolic risk measures and the sleep-disordered breathing parameters on the pooled study 1 and study 2 populations. Analyses on SBP and DBP were performed on the original scale, and analyses on hsCRP, HDL-C, non-HDL-C, triglycerides and HOMA-IR were performed on the log scale. These results are presented in Extended Data Table 1.
Ethics and informed consent
The study was approved by ethics review boards at each site, presented in Supplementary Table 1.
This study was conducted in accordance with consensus ethical principles derived from international guidelines including the Declaration of Helsinki and Council for International Organizations of Medical Sciences International Ethics Guidelines, applicable ICH GCP Guidelines, International Organization for Standardization (ISO) 14155 and applicable laws and regulations.
Participants or their legally authorized representatives signed a statement of informed consent that meets the requirements of 21 Code of Federal Regulations 50, local regulations, ICH guidelines, privacy and data protection requirements, where applicable, and the IRB/IEC or study center.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this Article.