
Study design, baseline clinicopathological characteristics and demographics
Table of Contents
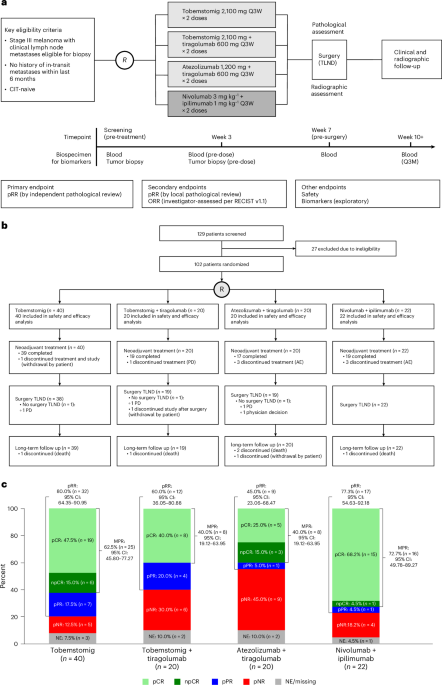
Morpheus-Melanoma was designed with the flexibility to open new treatment arms as new therapies became available, to close existing treatment arms that demonstrated minimal clinical activity or unacceptable toxicity or to expand enrollment in an experimental arm after promising initial signals. Patients 18 years of age or older with clinically detectable, RECIST-measurable, resectable stage III melanoma, with Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1 and no history of in-transit metastases within the last 6 months or prior radiotherapy or systemic cancer therapy for their disease, were randomized to receive preoperative tobemstomig, tobemstomig plus tiragolumab, atezolizumab plus tiragolumab or nivolumab plus ipilimumab (Fig. 1a).
aEligible patients were randomized to receive one of the following neoadjuvant treatments Q3W for 6 weeks: tobemstomig 2,100 mg, tobemstomig 2,100 mg plus tiragolumab 600 mg, atezolizumab 1,200 mg plus tiragolumab 600 mg or control treatment of nivolumab 3 mg kg−1 plus ipilimumab 1 mg kg−1. Randomization was stratified by geographic region (Australia versus rest of the world) and baseline LDH (≤ULN versus >ULN). Therapeutic lymph node dissection occurred at week 7, and pathological response was evaluated according to INMC criteria. Tumor biopsies were obtained prior to treatment and at week 3 (pre-dose). Blood was collected for biomarker evaluation pre-treatment, at week 3, at the time of TLND (pre-TLND, week 7) and post-TLND at weeks 10 and 13. Dark gray denotes the control arm (nivolumab plus ipilimumab). bPatient disposition by treatment arm, showing screening, randomization, completion of neoadjuvant therapy, TLND and long-term follow-up. cBreakdown of pathological responses for the efficacy-evaluable population (n = 102). Pathological response by independent pathological review occurred in 32 patients (80.0%) in the tobemstomig arm, in 12 patients (60.0%) in the tobemstomig plus tiragolumab arm, in nine patients (45.0%) in the atezolizumab plus tiragolumab arm and in 17 patients (77.3%) in the nivolumab plus ipilimumab arm. pCR is defined as 0% viable tumor cells; npCR is defined as ≤10% viable tumor cells; pPR is defined as >10% to ≤50% viable tumor cells; and pNR is defined as >50% viable tumor cells. 95% CIs for rates were calculated using the Clopper–Pearson method. AE, adverse event; CI, confidence interval; CIT, cancer immunotherapy; NE, not evaluable; PD, progressive disease; Q3M, every 3 months; Q3W, every 3 weeks.
The primary efficacy endpoint was pRR, defined as the percentage of pathological complete response (pCR), near pathological complete response (npCR) and pathological partial response (pPR), at the time of surgery, by independent pathological assessment. The secondary efficacy endpoints were pRR by local pathological assessment and investigator-assessed overall RECIST response rate (ORR). In addition, MPR (defined as pCR + npCR) was assessed. Safety endpoints included immune-related adverse events and delayed surgery. Exploratory biomarker analyses were performed.
Overall, 102 patients with stage III melanoma (excluding patients with mucosal and uveal melanoma or acral melanoma and/or in-transit metastases within 6 months prior to screening) were enrolled between 2 February 2022 and 8 August 2023. Forty patients were enrolled in the tobemstomig arm, which was expanded based on the totality of efficacy and safety data using prespecified criteria at interim analyses; 20 patients were enrolled in the tobemstomig plus tiragolumab arm; 20 patients were enrolled in the atezolizumab plus tiragolumab arm; and 22 patients were enrolled in the control arm of nivolumab plus ipilimumab, which was open throughout the study (Fig. 1b). Of the 102 enrolled patients, 94 (92.2%) completed the treatment period: 39 (97.5%) in the tobemstomig arm, 19 (95.0%) in the tobemstomig plus tiragolumab arm, 17 (85.0%) in the atezolizumab plus tiragolumab arm and 19 (86.4%) in the nivolumab plus ipilimumab arm. One patient in the tobemstomig arm withdrew from the study; one patient in the tobemstomig plus tiragolumab arm discontinued due to disease progression prior to surgery; and three patients each in the atezolizumab plus tiragolumab and nivolumab plus ipilimumab arms discontinued due to adverse events.
Most patients were White (76.5%) and male (66.7%), and patient age was 25–81 years across arms (Table 1). The median baseline target lesion sum of diameters was consistent across arms (Table 1).
At study closure (28 May 2024), median follow-up was 11.2 months in the tobemstomig arm, 15.2 months in the tobemstomig plus tiragolumab arm, 11.8 months in the atezolizumab plus tiragolumab arm and 13.6 months in the nivolumab plus ipilimumab arm.
Efficacy
Pathological response
The efficacy-evaluable population comprised all 102 patients. Pathological response by independent pathological review occurred in 32 patients (80.0%) in the tobemstomig arm, in 12 patients (60.0%) in the tobemstomig plus tiragolumab arm, in nine patients (45.0%) in the atezolizumab plus tiragolumab arm and in 17 patients (77.3%) in the nivolumab plus ipilimumab arm (Figs. 1c and 2A and Supplementary Table 1). In the tobemstomig arm, 19 patients (47.5%) had pCR, six patients (15.0%) had npCR (MPR 62.5%) and seven patients (17.5%) had pPR. In the tobemstomig plus tiragolumab arm, eight patients (40.0%) had pCR (MPR 40.0%) and four patients (20.0%) had pPR. In the atezolizumab plus tiragolumab arm, five patients (25.0%) had pCR, three patients (15.0%) had npCR (MPR 40.0%) and one patient (5.0%) had pPR. In the nivolumab plus ipilimumab arm, 15 patients (68.2%) had pCR and one patient each (4.5% each) had npCR (MPR 72.7%) and pPR. Pathological response by independent and local assessment was consistent (Extended Data Fig. 1 and Supplementary Table 1).

aPathological response by independent pathological review, according to INMC guidelines, plotted as a waterfall showing the area of non-viable tumor bed at the time of surgery, alongside pre-treatment biomarkers, including BRAF mutation status, TMB, IHC, IF and RNA-seq. Patients with pCR are ordered according to tumor inflammation, as determined by the mean rank of all TME biomarkers shown. bPre-treatment prevalence of selected immune biomarkers in the TME of patients across treatment arms (n = 79 patients with IHC data). The box plots illustrate the distribution of biomarker levels, showing the median (central line), interquartile range (box) and data range (whiskers, up to 1.5 times the interquartile range). Asterisks denote statistically significant differences between arms (two-sided rank-sum test; see legend). cAssociation between pre-treatment immune TME biomarkers and MPR (n = 87 patients with baseline data). The color gradient represents the area under the ROC curve (AUC), with values ranging from 0.5, indicating random prediction, to 1.0, indicating perfect prediction accuracy. Statistical significance is indicated using asterisks as defined in the legend (two-sided rank-sum test with Benjamini–Hochberg multiple testing correction). dImprovement in predictive performance using composite scores of pre-treatment immune biomarkers combined with TMB. Stacked bar plots display the AUC for individual immune biomarkers (blue) and the enhanced AUC achieved by integrating these biomarkers with TMB into composite scores (red). IF, immunofluorescence; MB, megabase; NK; natural killer; ROC, receiver operating characteristic; TC, tumor cell; TIC, tumor-initiating cell.
ORR
The investigator-assessed ORR (per RECIST version 1.1) was 37.5% in the tobemstomig arm, 60.0% in the tobemstomig plus tiragolumab arm, 35.0% in the atezolizumab plus tiragolumab arm and 59.1% in the nivolumab plus ipilimumab arm (Extended Data Fig. 2). In general, ORR and pathological responses were concordant; however, radiographic assessment underestimated pathological response in some patients (Extended Data Fig. 2).
Safety
The safety-evaluable population comprised all 102 patients. Overall, 36 patients (90.0%) in the tobemstomig arm, 18 patients (90.0%) in the tobemstomig plus tiragolumab arm, 19 patients (95.0%) in the atezolizumab plus tiragolumab arm and 19 patients (86.4%) in the nivolumab plus ipilimumab arm experienced at least one adverse event of any grade (Table 2). Time to onset and duration of each grade 3 or higher adverse event are provided in Supplementary Table 2.
TRAEs were experienced by 34 patients (85.0%) treated with tobemstomig, by 17 patients (85.0%) treated with tobemstomig plus tiragolumab, by 15 patients (75.0%) treated with atezolizumab plus tiragolumab and by 18 patients (81.8%) treated with nivolumab plus ipilimumab. The most common TRAEs (≥20% in any arm) were fatigue (30.0% versus 25.0% versus 15.0% versus 31.8%), hyperthyroidism (17.5% versus 30.0% versus 15.0% versus 18.2%), rash (17.5% versus 10.0% versus 5.0% versus 27.3%), pruritus (15.0% versus 15.0% versus 5.0% versus 36.4%) and asthenia (5.0% versus 5.0% versus 20.0% versus 9.1%) in the tobemstomig, tobemstomig plus tiragolumab, atezolizumab plus tiragolumab and nivolumab plus ipilimumab arms, respectively.
One patient (2.5%) in the tobemstomig arm, three patients (15.0%) in the tobemstomig plus tiragolumab arm, no patients in the atezolizumab plus tiragolumab arm and five patients (22.7%) in the nivolumab plus ipilimumab arm experienced a grade 3 or higher TRAE. There were no treatment-related deaths in any of the treatment arms.
Protocol-predefined immune-mediated adverse events are described in Table 2 and Supplementary Table 3.
Therapeutic lymph node dissection rates
There were 38 patients (95.0%) treated with tobemstomig, 19 patients (95.0%) treated with tobemstomig plus tiragolumab, 18 patients (90.0%) treated with atezolizumab plus tiragolumab and 22 patients (100%) treated with nivolumab plus ipilimumab who underwent a therapeutic lymph node dissection (TLND). TLND was performed within 2 weeks of the second cycle of neoadjuvant therapy, as scheduled, for most patients in each arm but was delayed by more than 2 weeks in eight patients (Table 2). TLND was not performed in five patients due to progressive disease (one patient each in the tobemstomig, tobemstomig plus tiragolumab and atezolizumab plus tiragolumab arms), patient withdrawal (one patient in the tobemstomig arm) and physician decision (one patient in the atezolizumab plus tiragolumab arm). Of the eight patients who had TLND delayed by more than 2 weeks, most delays were due to adverse events. Adverse events leading to TLND delay were hyperthyroidism and a SARS-CoV-2-positive test in the tobemstomig arm (one patient each), hyperthyroidism in the tobemstomig plus tiragolumab arm (one patient) and aseptic meningitis, pneumonitis and tachycardia in the nivolumab plus ipilimumab arm (one patient each). No patients in the atezolizumab plus tiragolumab arm had TLND delayed by more than 2 weeks.
Biomarkers
Baseline tumor microenvironment biomarker distributions by treatment arm
Overall, 90 of 102 patients (88.2%) had pre-treatment biopsies with sufficient tumor content for baseline biomarker evaluation. At study entry, canonical markers of an inflamed tumor microenvironment (TME), such as PD-L1 protein and gene expression and CD3+ and CD8+ T cell density in tumor stroma and tumor nests, were lower in patients in the tobemstomig arm versus the nivolumab plus ipilimumab arm (Fig. 2a,b and Extended Data Fig. 3). Tumor mutational burden (TMB; evaluated only in patients treated with tobemstomig and nivolumab plus ipilimumab based on favorable efficacy results) and the prevalence of BRAF V600E and V600K mutations were similar in patients in the tobemstomig arm and the nivolumab plus ipilimumab arm. The level of baseline tumor T cell infiltration was similar for patients enrolled in the tobemstomig and tobemstomig plus tiragolumab arms.
Association of baseline TME biomarkers and pathological response
Several baseline immune features in the TME were associated with pathological response to treatment. In the tobemstomig arm, baseline tumor-infiltrating CD8+ T cell density (in tumor nests and stroma), CD3+ T cell density, LAG-3 protein expression, immune-related genes and gene signatures (including LAG-3, PDCD1CD274, CD8 TeffIFNγ pathway and major histocompatibility complex (MHC) pathway) were associated with MPR (P < 0.05) (Fig. 2cExtended Data Fig. 4 and Supplementary Fig. 1). Similar associations were observed with the other treatments (Fig. 2cExtended Data Fig. 4 and Supplementary Fig. 1) and were consistent irrespective of the response threshold (MPR or any pathological response; Extended Data Fig. 5 and Supplementary Fig. 2).
BRAF V600E mutation status was not associated with pathological response to any treatments, although there was a trend for a greater proportion of non-responders in patients with BRAF V600E versus others in the tobemstomig arm (Fig. 2A). Among the seven patients with BRAF V600K mutations, five were pathological responders, one was a pathological non-responder and one had no pathological response evaluation. Patients with BRAF V600K mutations had similar levels of baseline tumor CD8 T cell infiltration to patients with BRAF V600E mutations.
Immune-related genes and proteins indicative of TME inflammation were correlated at baseline and were independent of TMB (Extended Data Fig. 6). TMB was associated with pathological response to tobemstomig, albeit to a lesser degree than other inflammatory TME immune biomarkers evaluated (Fig. 2c and Extended Data Fig. 7). The predictive potential of individual biomarkers improved when combined with TMB (Fig. 2D and Extended Data Fig. 8).
Immune cell dynamics in the TME
Paired metastatic lymph node biopsies were obtained from 79 patients (77.5%) before and after one treatment cycle and were evaluated for pharmacodynamic biomarkers relevant to drug mode of action (MOA). In many patients, little to no viable tumor was observed in on-treatment biopsies obtained after a single treatment cycle at cycle 2, day 1 (C2D1). These patients demonstrated distinct histologic features, including extensive levels of fibrosis and immune infiltration, compared to others; ultimately, these patients were identified as MPR at the time of TLND (Fig. 3a,b).

Immune dynamics in the TME, relevant to the drug MOA, were evaluated in pre-treatment and on-treatment lymph node tumor tissue from patients with clinical stage III melanoma treatment with neoadjuvant immunotherapy. aRepresentative histologic H&E stains of metastatic pre-treatment and on-treatment tumor tissue from pNR and pCR patients after one cycle of tobemstomig treatment, demonstrating reduction in viable tumor and increases in fibrosis in a patient with pCR compared to a patient with pNR. bBox plot showing the percentage of viable tumor in pre-treatment and on-treatment tumor tissue from patients in each pathological response category after one treatment cycle (n = 79). Patients from different treatment arms are pooled. cHeatmap representation of changes in immune and tumor genes and gene signatures in the TME on-treatment compared to pre-treatment (left) with zoom out on the individual genes comprising stem-like T cells, IFNγ, Treg cells and melanoma gene signatures, respectively (right). Patients are grouped according to treatment. Statistical significance is indicated using asterisks as defined in the legend (two-sided rank-sum test with Benjamini–Hochberg multiple testing correction). dBox plot representation of IHC/IF-derived CD8+ T cell and FOXP3 density and CD8/FOXP3 ratio in pre-treatment and on-treatment metastatic tumor biopsies from patients treated with tobemstomig (n = 13) or nivolumab plus ipilimumab (n = 8). e,fPooled analysis across all study treatments of CD8 T cell dynamics on-treatment according to pathological response. CD8 Teff and stem-like CD8 T cell signatures were derived from tumor bulk RNA-seq (n = 79) (e), whereas CD8+ and CD3+Perforin+ T cell densities were assessed by IHC and IF, respectively (n = 32) (f). Box plots illustrate the median (central line), interquartile range (box) and minima and maxima (whiskers, up to 1.5 times the interquartile range), with data points beyond this limit shown as individual outliers. Individual patients (dots) are colored by pathological response. FC, fold change; PRF1, Perforin; IF, immunofluorescence; NK; natural killer; TC, tumor cell.
Treatment led to the upregulation of immune-related gene signatures in the TME (IFNγ pathway, CD8 TeffMHC pathway) and downregulation of melanoma-associated gene signatures after one treatment cycle. The most notable transcriptional changes in the TME on-treatment were observed with tobemstomig and nivolumab plus ipilimumab (Fig. 3c and Supplementary Fig. 3).
To evaluate the proposed MOA of tobemstomig to reinvigorate TILs and bypass Treg cells in the TME, relevant immune-related gene signatures were evaluated and compared to those elicited in response to nivolumab plus ipilimumab. CD8 Teff cells, stem-like T cells and IFNγ pathway gene signatures increased with tobemstomig and nivolumab plus ipilimumab treatment (P < 0.01) (Fig. 3c). Treg gene signatures increased with tobemstomig and nivolumab plus ipilimumab treatment (Fig. 3c and Supplementary Fig. 3). Consistent with gene expression data, CD8 TIL density (including in tumor nests and stroma) and proliferating (CD8+K67+) and cytotoxic (CD3+Perforin+) T cells increased with tobemstomig treatment (P < 0.05) (Fig. 3D and Supplementary Fig. 4). The ratio of CD8 to FOXP3 tended to increase with tobemstomig (not significant) but did not change with nivolumab plus ipilimumab treatment (Fig. 3D).
No significant differences were observed in immune cell dynamics after tobemstomig versus tobemstomig plus tiragolumab treatment, based on tumor whole transcriptome.
Because all CPIs evaluated in this study aim to reinvigorate TILs, and to overcome the limited sample size within individual treatment arms, we pooled patients across treatments and evaluated the association between tumor-infiltrating T cell dynamics with pathological response. In general, responders had higher on-treatment immune gene and protein expression versus non-responders. Interestingly, some patients with low or medium levels of baseline CD8 T cell density and gene expression showed robust increases on-treatment, in absence of clinical benefit (that is, were pathological non-responders (pNR)), potentially reflecting underlying T cell intrinsic or extrinsic resistance mechanisms that may hinder generation of an effective antitumor immune response (Fig. 3e, f and Extended Data Fig. 9).
Circulating tumor DNA dynamics
Circulating tumor DNA (ctDNA) was evaluated over time in patients treated with tobemstomig and nivolumab plus ipilimumab (n = 39), based on the favorable efficacy observed for these treatments compared to others. Pre-treatment ctDNA was detected in 35 of 39 patients (89.7%), despite early disease stage.
Among patients with detectable ctDNA at baseline, 68% of those with a pathological response (21/31: pCR 17/22; npCR 3/4; pPR 1/5) achieved ctDNA clearance by week 7 pre-surgery versus one of four patients (25%) with pNR (Fig. 4A and Extended Data Fig. 10a). Furthermore, ctDNA clearance was observed in 50.0% (11/22) of patients with pCR after one cycle of CPI treatment and increased to 77.3% (17/22) after two cycles of CPI treatment.

Longitudinal ctDNA dynamics assessed over time in patients treated with tobemstomig or nivolumab plus ipilimumab. aSwimmer plot depicting ctDNA status over patient visit from screening (pre-treatment), C2D1, week 7 (pre-surgery) and weeks 10 and 13 (post-surgery) (n = 39). Patients are grouped by treatment and ordered by pathological response within each treatment group. Purple arrow indicates the time of TLND (week 7). bBox plot representing change in ctDNA levels at the pre-surgery timepoints, C2D1 and week 7, compared to pre-treatment levels for pathological response categories (n = 39). Ratio represents the mean tumor molecules per milliliter of plasma at on-treatment compared to baseline. Patients from different treatment arms are pooled. Box plots illustrate the median (central line), interquartile range (box) and minima and maxima (whiskers, up to 1.5 times the interquartile range), with data points beyond this limit shown as individual outliers. Individual patients (dots) are colored by pathological response. SCRN, screening; WK, week.
In patients with pCR and npCR, with no ctDNA clearance prior to surgery, significant decreases in ctDNA were nevertheless observed in all cases at week 7 (100%) versus pre-treatment levels. Patients with pCR had lower on-treatment ctDNA levels relative to baseline compared to other patients (C2D1: P = 0.01; week 7: P = 0.09) (Fig. 4B).
Pre-surgery ctDNA longitudinal dynamics were similar in patients treated with tobemstomig and nivolumab plus ipilimumab (C2D1: P = 0.95; week 7: P = 0.97) (Extended Data Fig. 10b) and correlated with the percentage of non-viable tumor deposits at the time of surgery (C2D1: r = −0.45, P = 0.0061; week 7: r = −0.61, P < 0.0005) (Extended Data Fig. 10c) and with radiographic response by RECIST at week 6 (C2D1: r = 0.64, P < 0.005) (Extended Data Fig. 10d).
Most patients with detectable ctDNA at baseline were ctDNA negative after surgery, both at week 10 and at week 13, with no disease recurrence. The only exception was one patient with pNR with an increase in ctDNA levels at week 13 and concomitant disease recurrence (Fig. 4A and Extended Data Fig. 10b). Among patients with no detectable ctDNA at baseline (4/39: three pCR, one pPR), all remained ctDNA negative throughout the subsequent visits evaluated.