
Phase 2b clinical trial
Table of Contents
- Phase 2b clinical trial
- Mediation analysis of the contribution of weight loss to MASH improvement
- Correlation between MASH resolution and improvement in features of the metabolic syndrome
- SomaScan proteomic profiling and SomaSignal NASH tests in participants with biopsy-confirmed MASH
- SomaScan assay
- SomaSignal NASH tests
- Individual SomaScan markers changing with semaglutide treatment
- Semaglutide proteomic signature
- Effect of semaglutide on Hallmark gene sets
- Biomarkers mediating the semaglutide effect on MASH resolution
- Protein mediators of the semaglutide effect on MASH resolution separate of weight loss
- Change in proteomic mediators in participants with biopsy-confirmed MASH in the independent cohort
- Semaglutide treatment in DIO-MASH and CDA-HFD mice: effects of treatment duration on liver fibrosis
- Semaglutide treatment in DIO-MASH and CDA-HFD mice
- DIO-MASH study
- CDA-HFD study
- Sampling and histology
- Liver histology and image analysis
- Next-generation RNA sequencing
- GLP-1 receptor expression in mouse and human liver
- Reporting summary
The data and analyses derive from a 72-week, multicenter, randomized, parallel-group trial of semaglutide versus placebo, the results of which were published in detail previously5. In brief, this trial involved 320 adult participants (18–75 years of age (20–75 years of age in Japan)), with or without T2D and a body mass index higher than 25 kg m−2 at screening with histological evidence of MASH (defined as the presence of at least grade 1 steatosis, lobular inflammation and hepatocyte ballooning with an overall non-alcoholic fatty liver disease activity score (NAS) of 4 or higher) and a fibrosis stage of F1, F2 or F3 based on the Kleiner fibrosis classification. NAS and the fibrosis stage were assessed centrally by two independent expert hepatologists who were blinded to treatment assignment, patient characteristics and each other’s assessment. In case of different opinions on any variable, diagnostic agreement was reached through a consensus call.
Liver-related exclusion criteria were documented causes of chronic liver disease other than MASH, in particular hepatitis B (including positive hepatitis B surface antigen), hepatitis C (including positive HCV-RNA) and alcoholic liver disease or known or suspected abuse of alcohol (>20 g per day for women or >30 g per day for men), alcohol or narcotics dependence assessed by the Alcohol Use Disorders Identification Test (AUDIT questionnaire), liver transplantation, elevated liver tests (liver enzymes >5 times the upper normal limit, elevated total bilirubin (>1.5 mg dl−1) and international normalized ratio >1.3) and treatment with vitamin E or pioglitazone that has not been at a stable dose in the period for 90 days prior to screening or from historical baseline biopsy until screening, respectively. Glucose-related and obesity-related exclusion criteria included glycated hemoglobin (HbA1c) > 10% at screening, treatment with GLP-1RAs or sodium/glucose co-transporter 2 inhibitors in the period from 90 days prior to screening or from historical baseline biopsy until screening, treatment with any other glucose-lowering agent not stable in the period from 28 days prior to screening or from historical baseline liver biopsy until screening, participation in an organized weight reduction program, previous surgical treatment for obesity and any treatment with a medication that could promote weight loss.
Participants, stratified by geographic region, T2D status and fibrosis stage, were randomized to receive semaglutide at a maximum dose of 0.1 mg (n = 80), 0.2 mg (n = 78) or 0.4 mg (n = 82) or placebo (n = 80) via once-weekly subcutaneous injection for 72 weeks. Biopsy samples obtained at screening were used as baseline for histologic variables, and an additional biopsy was obtained at week 72. In addition to per-protocol laboratory analyses, human biosamples for future analysis were retained, as long as participants had signed a separate informed consent form. Stored fasting serum from participants was used to perform large-scale proteomic profiling using the SomaScan multiplex affinity assay.
This trial accorded with the ethical principles of the Declaration of Helsinki and was consistent with the International Conference on Harmonization of Good Clinical Practice and applicable regulatory requirements. The protocol was approved by the institutional review board and ethics committee at each participating trial site5. Participants provided written informed consent for use of biosamples for future research, and the ethics committees approved the specific use of the biosamples.
In total, 94% (n = 302) of participants completed the trial (that is, accomplished the final trial visit), and 89% (n = 285) completed treatment. In 87% (n = 277) of randomized participants, liver biopsy at week 72 was available to evaluate the primary endpoint of resolution of MASH and the confirmatory secondary endpoint of improvement of at least one fibrosis stage and no worsening of MASH. Outcomes were calculated with missing values imputed as non-responders.
Among participants included in this trial, 61% (n = 193) were women, 78% (n = 248) were White and 13% (n = 40) were Hispanic or Latino. In total, 51% (n = 163) of trial participants were enrolled in Europe and Australia, 36% (n = 116) in North America and 13% (n = 41) in Japan.
Baseline demographics and disease characteristics were generally similar across treatment groups. Mean participant age was 55 years; mean body weight was 98.4 kg; and mean body mass index was 35.8 kg m−2. One hundred sixty-five out of 320 randomized patients (52%) had a body mass index of 35 kg m−2 or higher.
Mediation analysis of the contribution of weight loss to MASH improvement
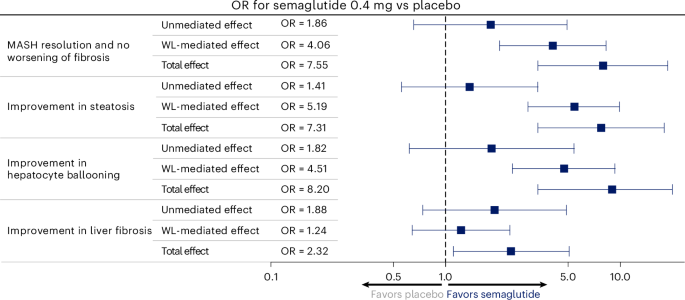
To investigate whether semaglutide improved liver histology through weight loss or via mechanisms separate from weight, mediation analyses using natural effects models were performed. The analyses were based on complete-case on-treatment measurements (N = 249) for histological parameters that showed a statistically significant effect of semaglutide. Changes from baseline in weight at all nine scheduled visits were used as a mediator. The model was adjusted for baseline body weight, fibrosis stage, T2D status, age and gender. The analyses assessed the mediated (weight-loss-dependent) and non-mediated (after adjusting for weight change—that is, separate from weight loss) effects of treatment on liver histology. Results are presented as the mediated proportion—that is, the indirect/weight-loss-dependent effect divided by the total effect, with corresponding CIs. Covariates were imputed using single imputation based on predicted value/response from a mixed model for repeated measurements (MMRM). The mediation analysis was performed using the ‘medflex’ package in R.
Correlation between MASH resolution and improvement in features of the metabolic syndrome
Changes in features of the metabolic syndrome at week 72 are presented by treatment and MASH resolution response at week 72 using descriptive statistics based on the on-treatment observation period. To investigate the efficacy of semaglutide on the metabolic and inflammatory features, post-baseline changes were analyzed using an MMRM, with baseline diabetes status, baseline fibrosis stage and diabetes-by-fibrosis interaction as factors (HbA1c, fasting plasma glucose, homeostatic model assessment of insulin resistance, adipose tissue insulin resistance and non-high-density lipoprotein cholesterol could not be included in the diabetes-by-fibrosis interaction as factors) and baseline body weight and baseline value of the feature as covariates, all nested within visit. All scheduled post-baseline assessments during the on-treatment period were used in the model.
SomaScan proteomic profiling and SomaSignal NASH tests in participants with biopsy-confirmed MASH
Serum samples for future use were obtained at four timepoints in the phase 2 trial: at baseline and after 28, 52 and 72 weeks of treatment. For some participants, samples were not shipped to SomaLogic for analysis due to lack of consent or availability of samples in the storage facility upon the cutoff date for the use of samples. After preprocessing and quality control of the SomaLogic data, a total of 10 serum samples failed. Thus, 1,088 serum samples were included in the SomaLogic analyses, representing 293 of the enrolled 320 participants.
SomaScan assay
The SomaScan protein array v.4 profiled 4,979 different proteins. Standard preprocessing of the SomaScan array data was performed in accordance with guidance from SomaLogic. The relative fluorescence units (RFU) from each sample were normalized based on (1) hybridization controls on each microarray to correct for systematic variability in hybridization and (2) median signal based on all features for each dilution to correct for variability across plates according to the SomaScan Data Standardization guidelines (SomaScan Data Standardization and File Specification Technical Note (SSM-020)). All RFUs were natural logarithm transformed for uniformity.
SomaSignal NASH tests
The protein expression levels measured using the SomaScan protein array were used for the multi-protein SomaSignal NASH tests. The SomaSignal NASH tests provide categorizations of participants for each of the four MASH components: steatosis, hepatocyte ballooning, lobular inflammation and fibrosis. An overview of the individual proteins from the SomaScan protein array that are included in each of the four SomaSignal NASH tests is presented in Supplementary Table 1. SomaSignal NASH tests used predicted probabilities (continuous score from 0 to 1), with the higher the predicted probability, the higher the likelihood of elevated NAS component and fibrosis stage. Predicted probability was used to categorize the test as positive or negative based on a decision threshold of 0.5 (validated for identification of stage: steatosis ≥1, inflammation ≥2, ballooning ≥1 and fibrosis ≥2). In a subgroup analysis, changes in predicted probabilities were analyzed by an MMRM based on on-treatment data. The proportion of patients with improvement was defined as negative SomaSignal NASH test (predicted probability <0.5 on a 0–1 scale) at week 72.
Individual SomaScan markers changing with semaglutide treatment
An MMRM was used with treatment, baseline diabetes status, baseline fibrosis stage and diabetes-by-fibrosis interaction as factors and baseline body weight and baseline value of the biomarker as covariates, all nested within visit. Statistical significance was based on a Bonferroni-adjusted alpha level of 0.1 for the treatment ratio at week 72 of semaglutide 0.4 mg once daily/placebo.
Semaglutide proteomic signature
A protein signature was developed for the semaglutide treatment effect (0.4 mg versus placebo; response variable in model). Data mining using the (repeated) LASSO procedure was done using all biomarkers as input. For each marker, change from baseline at week 72 was used (predictor variables). The average area under the concentration time curve for classifying semaglutide 0.4 mg versus placebo from internal cross-validation was 0.92.
Effect of semaglutide on Hallmark gene sets
A gene set enrichment analysis was performed. As input, model estimates were used for the treatment ratio at week 72, semaglutide 0.4 mg/placebo, for all 4,979 protein biomarkers.
Biomarkers mediating the semaglutide effect on MASH resolution
To identify protein biomarkers that statistically mediate the effect of semaglutide on MASH resolution, two models were fitted for all 4,979 proteins. First, we used a linear regression model of semaglutide treatment versus protein change at week 72. Second, we used a logistic regression model of protein change versus MASH resolution, both at week 72. The same covariates were included as in the MMRM. P values from both models were combined, following the classical framework for causal mediation, to compute a false discovery rate (FDR)-adjusted mediation P value following the procedure by Dai et al.37.
Protein mediators of the semaglutide effect on MASH resolution separate of weight loss
We used two procedures to identify whether the protein mediators for the effect of semaglutide on MASH resolution are separate from change in body weight. First, a linear regression was fitted for the association of protein change versus change in body weight, both at week 72. The same covariates were included as in the MMRM. We used a P > 0.05 threshold to indicate independence. Second, we repeated the above procedure using two models that included baseline body weight and weight change at week 72 as covariates in the model. Markers that had P < 0.05 for both models were considered to mediate separate from body weight.
Change in proteomic mediators in participants with biopsy-confirmed MASH in the independent cohort
The independent CoCoMASLD cohort comprised patients with MASLD referred to a single gastroenterology department in Denmark. The patient subset included the initially recruited patients who underwent a biopsy and were included in proteomic analyses as well as healthy controls. Patients were diagnosed as having MASH based on histopathological evaluation. The pathologists provided NASH Clinical Research Network scores for steatosis and fibrosis but only yes/no for lobular inflammation and ballooning. Hence, the patients could not be assigned a NAS. Patients were diagnosed with MASH when all three features (steatosis, lobular inflammation and ballooning) were observed in the liver biopsy
The SomaScan v.4.1 (7k) platform was used to generate SomaLogic data from serum samples. RFU computed by adaptive normalization by maximum likelihood were provided by the vendor. Samples that did not pass vendor quality control thresholds were removed. Likewise, aptamers classified as non-human or non-proteins or with median RFU below the lower limit of detection were excluded from the analysis. Differential gene expression analysis was performed using the limma v.3.52.1 R package38. A linear model was fit using lmFit on log2 RFU while adjusting for age, sex, body mass index and diabetes status. The eBayes function was used to compute moderated t-statistics by setting trend and robust parameters to true. CIs were computed using the limma ‘topTable’ function, setting a Bonferroni-corrected threshold of 0.05. Aptamer log2 fold changes and corresponding CIs were joined with the results from the mediation analysis based on SomaLogic sequence identifiers. Box plots of protein abundance across healthy and MASH samples were based on log2 RFU after removing effects from gender, age, diabetes and body mass index using the limma function ‘RemoveBatchEffect’.
Semaglutide treatment in DIO-MASH and CDA-HFD mice: effects of treatment duration on liver fibrosis
The Danish Animal Experiments Inspectorate approved all experiments, which were conducted using internationally accepted principles for the use of laboratory animals (license no. 2013-15-2934-00784 and no. 2018-15-2934-00784 (Gubra) and no. 2017-15-0201-01215 (Novo Nordisk)). Each animal was identified by an implantable subcutaneous microchip (PetID Microchip; E-vet).
DIO-MASH studies
C57BL/6JRj mice (5–6 weeks old) were obtained from Janvier Labs and housed in a controlled environment (12-hour light/dark cycle, 21 ± 2.0 °C, humidity 50 ± 10%). Mice had ad libitum access to tap water and Gubra Amylin NASH diet (4.49 kcal g−140 kcal % fat; of these, 46% saturated fatty acids by weight, 22% fructose, 10% sucrose, 2% cholesterol; Research Diets, D09100310) for 34 weeks for the efficacy trial. In both DIO-MASH studies, a group was maintained on regular mouse chow (2.85 kcal g−1; Brogaarden, Altromin 1324) for comparison. A liver biopsy was taken from the mice 4 weeks before treatment start, as described in detail previously39,40,41. In brief, for pretreatment liver biopsy, mice were anesthetized with isoflurane; a small abdominal incision in the midline was made; and the left lateral lobe of the liver was exposed. A cone-shaped wedge of liver tissue (50–100 mg) was excised from the distal part of the lobe. The cut surface of the liver was closed by electrosurgical bipolar coagulation using an electrosurgical unit (ERBE VIO 100C; ERBE). The liver was returned to the abdominal cavity; the abdominal wall was sutured; and the skin was stapled. Intraperitoneal carprofen (5 mg kg−1) was administered at the time of surgery and at postoperative days 1 and 2. After the procedure, animals were single-housed and allowed to recover for 4 weeks prior to treatment start. Only mice with steatosis score 3 or mice with fibrosis score >1 and steatosis score >2 were included in the efficacy trial, as outlined by Kleiner et al.39. Included animals were then randomized into treatment groups based on mean baseline PSR area% 1 week before dose start.
CDA-HFD diet study
Male C57BL/6JRj mice (7–8 weeks old) were obtained from Taconic and housed in a controlled environment (12-hour light/dark cycle, lights on at 6:00, 21 ± 1.0 °C, humidity 45–65%). Mice had ad libitum access to tap water and either chow or a high-caloric CDA-HFD diet (kcal %: fat 60%, carbohydrates 20%; 5.2 kcal g−1; Research Diets, A06071302) for 6 weeks prior to treatment start.
Semaglutide treatment in DIO-MASH and CDA-HFD mice
Formulations
Semaglutide and vehicle were prepared at Novo Nordisk in Måløv, Denmark. Vehicle was PBS containing 0.007% polysorbate 20, 50 mM phosphate and 70 mM sodium chloride, at pH 7.4.
DIO-MASH study
In the efficacy study, animals were administered vehicle or semaglutide 123 µg kg−1 (n = 16) daily for 8, 16 or 24 weeks. Vehicle-dosed chow-fed mice (n = 10) served as additional controls.
Dosing was performed subcutaneously once daily in a volume of 5 ml kg−1. To reduce initial gastric discomfort, the dose was increased through daily increments until reaching the target dose on treatment day 5. The 123 µg kg−1 once-daily dose aimed to result in weight loss similar to that from a clinical dose of 2.4 mg/weekly, with adjustments for species differences in half-life. Body weight was monitored daily during the intervention period.
CDA-HFD study
CDA-HFD mice were randomly allocated to groups and treated with vehicle or semaglutide 20 µg kg−1 (n = 15) for 6 weeks or 12 weeks. A group of CDA-HFD mice was euthanized at treatment start to determine baseline levels of MASH (n = 10, baseline group). Vehicle-dosed chow-fed mice (n = 5) served as additional controls. Body weight was monitored every 3 days during the intervention period.
Sampling and histology
For histological analysis, a full-thickness slab of the left lateral lobe was fixed in 10% neutral buffered formalin and routine processed to paraffin blocks.
Liver histology and image analysis
Paraffin-embedded liver tissue was sectioned (nominal 4-µm thickness) and mounted on SuperFrost Plus slides. Sections of liver tissue were stained with hematoxylin and eosin (H&E), PSR, anti-αSMA (Abcam, ab124964 (0.4 µg ml−1) and ab5694 (0.2 µg ml−1)) or anti-type I collagen (Southern Biotech; Col1a1, 1310-01 (4 µg ml−1)) using standard procedures40. Quantitative histomorphometry was applied using digital imaging software (Visiomorph, Visiopharm). Fractional (%) area of liver fat (macrosteatosis) was determined on H&E-stained sections. PSR, αSMA and Col1a1 immunostaining was expressed as a fraction of the total parenchymal area without steatosis by subtracting the fraction of fat area determined on adjacent H&E-stained sections.
Next-generation RNA sequencing
All groups finishing the treatment phase were included in RNA sequencing analysis. Liver samples of 20 ± 10 mg were taken from the left lateral lobe, snap frozen in liquid nitrogen and stored at −70 °C. RNA was purified using a NucleoSpin Kit (Macherey-Nagel). Purified RNA (10 ng to 1 µg) from each sample was used to generate a cDNA library using an NEBNext Ultra II Directional RNA Library Prep Kit for Illumina. The cDNA library was then sequenced on a NextSeq 500 using NextSeq 500/550 High Output Kit V2 (Illumina).
The sequencing data were aligned to the mm10 (GRCm38) transcriptome, obtained from the Ensembl database, using STAR v.2.7.3a. Read counts were quantified by salmon v.1.2.0; read quality of the data was evaluated using FastQC 0.11.9 and Picard; and the intergroup and intragroup variability was evaluated using principal component analysis and hierarchical clustering. Differential gene expression was assessed by the R package DESeq2.
GLP-1 receptor expression in mouse and human liver
Human liver biopsies
Twenty-six human diagnostic, formalin-fixed, paraffin-embedded histological liver needle biopsies were retrieved from the archives at Aalborg Hospital in Denmark. The study was conducted in accordance with the ethical standards of the 1964 Declaration of Helsinki and its later amendments. It was checked that the participants had not stated in the Tissue Application Register (Vævsanvendelsesregisteret) at the Danish Data Protection Agency that biobanked material must not be used for research. The biopsies were fully anonymized, and it was not possible to identify the donors of the biobanked material.
GLP-1 receptor expression was assessed in human liver biopsies as described previously42,43 with some modifications. In short, the sections were microwave-treated in TEG buffer (pH 9.0) (Ampliqon) for 15 minutes and allowed to cool for 15 minutes. Slides were rinsed in tap water and treated with 1% H2O2 in Tris-buffered saline for 15 minutes and rinsed in Tris-buffered saline followed by avidin/biotin blocking. The sections were pre-incubated with 0.5% TNB blocking buffer (PerkinElmer) for 2 hours and incubated with the validated GLP-1 receptor monoclonal antibody (Mab 3F52) at 5 µg ml−1 (ref. 43) overnight at 4 °C in 0.5% TNB blocking buffer. The next day, sections were incubated with VECTASTAIN ABC (Vector Laboratories) and developed with DAB+ (Enzo Life Sciences). Slides were washed with Tris-buffered saline with 0.05% Tween between incubations.
In situ hybridization was performed on the human liver biopsies on a Ventana Discovery Ultra automation system (Ventana Medical Systems) using an RNAscope VS Universal HRP/AP Kit (Advanced Cell Diagnostics) and the specific GLP1R probe, RNAscope 2.5 VS Probe-Hs-GLP1R (Advanced Cell Diagnostics, cat. no. 519829). Positive (peptidylprolyl isomerase B, NM_011149.2) and negative (Bacillus Subtillis, dihydropicolinate reductase, EF191515) in situ hybridization control probes were employed for assay validation in all analyses.
Mouse liver
In mice, GLP-1 receptor expression was assessed using immunohistochemistry in three liver lobes from each of one chow/vehicle dosed and four DIO-NASH vehicle or CDA-HFD vehicle mice. The tissues were analyzed on the Ventana Discovery Ultra automation system (Ventana Medical Systems) for GLP-1 receptor expression using rabbit-anti-mGLP1R (Abcam, ab218532, lot: GR3231665-2) at a concentration of 2.7 µg ml−1. In brief, 5-µm sections were baked at 60 °C for 32 minutes and then deparaffinized at 72 °C for 24 minutes. Pretreatment in buffer CC1 was at 95 °C for 16 minutes, followed by incubation in HRP block for 12 minutes. After application of primary antibody, slides were incubated at 37 °C for 60 minutes and then detected with anti-rabbit HQ at 35 °C for 24 minutes, followed by anti-HQ HRP 35 °C for 16 minutes. Chromogen (Purple) was applied for 32 minutes, and then sections were counterstained with Hematoxylin II for 8 minutes and with bluing reagent for 4 minutes. Pancreas, duodenum, stomach and kidney were used as positive control tissues using the same automated immunohistochemistry protocol.
Statistics and reproducibility
The phase 2 clinical trial was powered to show a difference in proportions of 28% on primary endpoint MASH resolution and no worsening of fibrosis between once-daily semaglutide 0.4 mg (assumed 45% response) and placebo (assumed 17% response). The study was randomized (1:1:1:1: placebo; semaglutide 0.1 mg; semaglutide 0.2 mg; semaglutide 0.4 mg), and investigators and patients were blinded. For the proteomics analysis, no formal power calculation was conducted. However, all statistical proteomics analyses were rigorously adjusted for multiple testing using the FDR procedure. No data were excluded. For the mediation analysis on the histology endpoints evaluating change in body weight as mediator, data were based on complete-case on-treatment measurements to evaluate the mechanistic action of semaglutide in MASH (hence, data outside the on-treatment observation period were excluded). The estimated effects are presented along with 95% CIs (that is, not adjusted for multiplicity). The preclinical studies were powered based on power calculations on the endpoints with highest variability (alanine aminotransferase and Col1 area %) in previous studies. DIO-MASH animals with steatosis score ≥2 and a fibrosis stage of ≥1, based on liver biopsy taken 4 weeks before treatment start, were included. Animals were randomized into treatment groups on percentage fractional area of fibrosis (PSR staining) in the pretreatment biopsy. CDA-HFD animals were allocated to treatment groups without randomization. An age-matched control group on regular chow diet was included, without randomization. Data from animals that did not finish the study were excluded.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.